ARTICLE
Effectiveness of Population-Based Newborn Hearing
Screening in England: Ages of Interventions and
Profile of Cases
Kai Uus, MD, PhD, John Bamford, PhD
Audiology and Deafness Research Group, School of Psychological Sciences, Faculty of Medical and Human Sciences, University of Manchester, Manchester, United Kingdom
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.The objective of this study was to determine the effectiveness in routine practice of the first phase of a national population-based newborn hearing screen-ing and follow-up program that seeks to identify infants with bilateral permanent
hearing loss ofⱖ40-dB hearing loss.
METHODS.The study was a part of the independent evaluation of the 23 first phase
sites (annual birth population⬃120 000) of the national newborn hearing
screen-ing program in England. For each infant identified with the defined hearscreen-ing loss, the measures of interest were degree and type of hearing loss, presence of risk factors, age of first audiologic assessment, age of identification of hearing loss, age of enrollment in an early support program, and age of hearing aid fitting. Data collection took place over the first 2 years of the program.
RESULTS.Data were provided on 169 infants with permanent bilateral moderate or greater hearing loss identified through screening 169 487 infants. Fifty-four per-cent of all cases were from an “at-risk” population. Three fourths of these “at-risk”
infants spentⱖ48 hours in the NICU. For the whole sample, the median age at first
audiologic assessment was 5 weeks; the median age of identification of the hearing loss and of enrollment in early support program was 10 weeks irrespective of the degree of hearing loss; and the median age at hearing aid fitting was 16 weeks. Infants with moderate hearing loss were fitted with hearing aids significantly later than those with severe and profound hearing loss.
CONCLUSIONS.Properly implemented, a newborn hearing screening program based on whole populations and routine service provision can deliver satisfactory outcomes in terms of age of referral, identification, and intervention. The distribution of degree and type of hearing loss and proportion with risk factors was similar to that expected. The numbers identified were such as to suggest that very few cases were missed by the screening program.
www.pediatrics.org/cgi/doi/10.1542/ peds.2005-1064
doi:10.1542/peds.2005-1064 The views expressed in the publication are those of the authors and not necessarily those of the Department of Health. Key Words
newborn hearing screening, risk factors, age at identification, age at hearing aid fitting
Abbreviations
NHSP—newborn hearing screening program
CI— confidence interval OAE— otoacoustic emission ABR—auditory brainstem response WIN—well-infant nursery IQR—interquartile range
P
ERMANENT CONGENITAL BILATERAL hearing loss of moderate or greater degree is rare, with a prevalenceof around 1 per 1000 births.1However, there is evidence
that the impact of such hearing loss on the development of language and communication can be substantial un-less effective intervention is started within the first year
of life, preferably before 6 months of age.2 Language
development is positively and significantly affected by the age of identification of the hearing loss and age of initiation into intervention services. Although there re-mains some debate about the weight of evidence with regard to the effect of early intervention on language
development, largely because of study design issues,3
there are also cogent arguments for early identification
and intervention that derive from ethical principles.4
Before universal newborn hearing screening, the aver-age aver-age of identification of congenital permanent hear-ing loss was around 2 years in the United Khear-ingdom,
continental Europe, and North America,5–8and the
me-dian age of hearing aid fitting was delayed on average for
another 6 months.5
After a systematic review by Davis et al,9the
Depart-ment of Health in England commissioned a national population-based newborn hearing screening program (NHSP) in 2001. It is anticipated that all areas of England will participate in the program by late 2005. Simulta-neously, an independent evaluation of the first phase of the screen sites spread around the country covering
⬃120 000 births per annum was commissioned. The
evaluation showed an overall coverage of 96%, a mean referral rate of just below 3% (unilateral and bilateral referrals combined), a lost-to-follow-up rate of approx-imately 10%, and a yield for bilateral moderate or greater permanent hearing loss of 1.00 (95% confidence interval [CI] 0.78 –1.22) per 1000 screened (NHSP Eval-uation Team, unpublished data); the yield is in line with
the reported prevalence rate in England.5
Newborn hearing screening is merely the first step in comprehensive early hearing detection and intervention programs. To demonstrate effectiveness, a screening pro-gram requires that the services be in place to provide
authoritative follow-up and appropriate intervention.10
The aim of this part of the evaluation was to extend the data collection and analyses to the follow-up of infants referred by the screen to additional determine the effec-tiveness of the screen in routine practice. The number and type of hearing losses identified, the proportion with risk factors, and the ages of first audiologic assessment, identification, enrollment in early support program, and hearing aid fitting were chosen as the outcome mea-sures.
METHODS
The details of the screening protocol and screening sites
are reported elsewhere.11 Briefly, the NHSP
implemen-tation uses 2 screen protocols, 1 for well infants and 1 for
infants who have been in a NICU for ⱖ48 hours. Both
protocols involve 2 test procedures within the one screen. In the former, representing the great majority of screenings, well infants are tested using transient evoked automated otoacoustic emissions (OAEs) first and, if there is no clear emission in either ear, they undergo automated auditory brainstem response (ABR) testing. Thus, for well infants, the ABR test is contingent on the lack of clear OAE responses. For NICU infants, both OAE and ABR are used, with a screen refer if a clear response is missing on either (again, in either ear).
Procedure
Documentation for data collection was sent to the screening management teams of the 23 first phase NHSP sites shortly after each site had started the screening program. The documentation consisted of a detailed in-struction chart and 4 Proformas that the screening team leader was instructed to send to the pediatric audiology follow-up service(s) in their area. Three of the Proformas were completed by the pediatric audiology service and returned directly to the evaluation team. These Profor-mas were anonymized, displaying only the child’s local unique identifier and date of birth, and giving informa-tion on the 4 main measures (ages at first audiologic assessment, identification, enrollment in early support program, and hearing aid fitting), as well as gender, the degree and type of hearing loss, and presence of risk factors. The fourth Proforma, detailing the name, ad-dress, and local unique identifier of each true case, was sent by pediatric audiology services to the screening team leaders and retained by them.
Data were collected for all children born between the start of the screening program (variable across sites) and January 1, 2004, who were identified with permanent bilateral moderate or greater hearing loss (estimated
ⱖ40-dB hearing loss averaged over 0.5, 1, 2, and 4 kHz
in the better hearing ear). During this period, 169 487 infants were screened in the first phase NHSP sites that were spread all over England. Follow-up of referrals was undertaken by local pediatric audiology departments
working to preferred practice guidelines.12
Measures
Age at first audiologic follow-up is the chronologic age of the infant at the first audiologic follow-up assessment after a “screen-refer” decision. The data presented here are based only on the subjects who were eventually identified with hearing loss.
Age at identification is the chronologic age of the infant when, using age-appropriate assessments, there is good clinical evidence to suggest that the infant has a permanent bilateral moderate or greater hearing loss. At this stage, the exact degree and configuration of the hearing loss may still remain uncertain.
chronologic age of the infant when they are referred to the specialist education services that provide the pro-grams.
Age at hearing aid fitting is the chronologic age of the infant at the first hearing aid fitting.
Data Analysis
Analyses were conducted by using SPSS 11.5 for Win-dows (SPSS Inc, Chicago, IL). The main analyses con-sisted of 1-way analysis of variance comparing the
mea-sures for different degrees of hearing loss. Independentt
tests were conducted to compare measures for different types of nursery (well-infant nursery [WIN] versus NICU).
RESULTS
The number of cases that the evaluation team was in-formed of was 169. Considerable effort was put into reminding services to pass the information on cases to the evaluation team, and this figure is likely to be close to the “true” number identified. It gives a yield figure per thousand screened infants, which is close to published prevalence figures for congenital bilateral permanent
hearing loss of moderate or greater degree.1,5Of course,
some cases may still have not been identified as a result of, for example, assessment difficulties with mild to moderate losses or temporary conductive hearing loss overlay, nonattendance at follow-up, and so on (NHSP Evaluation Team, unpublished data). Nevertheless, the data presented in this section are likely to be robust and close to the “true” situation.
Profile of Cases
Tables 1 through 3 provide the basic information on the profile of the 169 infants identified with permanent bilateral hearing loss. Fifty-seven percent of the subjects were male and 43% were female.
As expected, sensorineural hearing loss was the most predominant type of hearing loss (Table 1). Auditory dyssynchrony was defined as a condition characterized by the absence or severe abnormality of ABR in the presence of OAEs and was reported in 17 cases. Fifty-four percent of the infants had identifiable risk factors. Table 2 details the distribution of risk indicators for these 91 infants. The most common indicator was spending
ⱖ48 hours in the NICU occasionally combined with a
family history of childhood hearing loss, craniofacial
anomaly, or both; 75.8% (N⫽69) of high-risk infants
were from the NICU population.
For the following analyses, subjects with auditory neuropathy have been excluded. Table 3 provides details of the distribution of degree of hearing loss (4-frequency average: moderate hearing loss 40 – 69-dB hearing loss; severe hearing loss 70 –94-dB hearing loss, and profound
hearing lossⱖ95-dB hearing loss).
Age at the First Audiologic Follow-up Assessment
Median age at the first follow-up appointment after
screen referral was 5 weeks. Independentttests showed
a significant difference in the age at the first audiologic follow-up assessment between infants from the WIN and
the NICU (t ⫽ 6.516; degrees of freedom ⫽ 139; P ⬍
.001), with the median age for WIN infants being 4 weeks (interquartile range [IQR] 3–10 weeks) compared with 9 weeks (IQR: 4.5–17 weeks) for NICU infants.
Table 4 details the descriptive statistics of the age at the first audiologic follow-up appointment for different degrees of hearing loss. Posthoc testing using the Tukey B test indicated that there was no significant difference in age at first follow-up between the different hearing
loss groups (F[2,130]⫽2.641;P⫽.075). When the data
from the NICU population were analyzed separately, the Tukey B test revealed a significant difference in age of first follow-up appointment between infants who were eventually identified with different degrees of hearing
loss (F[2,58]⫽4.132;P⫽.021): infants with profound
hearing loss fall into a separate subset for␣⫽.05, that is,
were followed up significantly later.
TABLE 1 Distribution of Type of Hearing Loss
Type N %
Permanent conductive 5 3.0
Mixed 7 4.1
Auditory dyssynchrony 17 10.1
Sensorineural 140 82.8
Total 169 100.0
TABLE 2 Distribution of Risk Factors in 91 High-Risk Infants Identified With Permanent Bilateral Hearing Loss
N %
NICU 58 63.7
FH 18 19.8
CF 4 4.4
NICU⫹CF 5 5.5
NICU⫹FH 4 4.4
NICU⫹FH⫹CF 2 2.2
Total 91 100.0
NICU indicates a history of admission to the NICU for⬎48 hours; FH, a family history of early childhood permanent deafness; CF, a craniofacial anomaly (eg, cleft palate) associated with permanent hearing loss.
TABLE 3 Distribution of Degree of Hearing Loss Based on Better Hearing Ear (nⴝ152)
Degree N %
Moderate 59 38.8
Severe 40 26.3
Profound 53 34.9
Total 152 100.0
Seventeen cases of auditory neuropathy have been excluded. Moderate hearing loss indicates 40 – 69-dB hearing loss; severe hearing loss, 70 –94-dB hearing loss; and profound hearing loss,
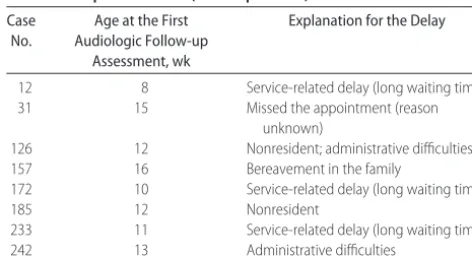
Table 5 gives details of the reasons for the delay for the first audiologic follow-up for WIN infants who emerged as statistical outliers. In NICU infants, the delay in attending first audiologic follow-up was without ex-ception to do with the health of the infant.
Age at Identification of Hearing Loss
Median age for identification of hearing loss was 10
weeks. Independent ttests showed a significant
differ-ence in the identification age between infants from WIN
and NICU (t ⫽2.638; degrees of freedom ⫽ 148;P ⫽
.009), with the median age for WIN infants being 10 weeks (IQR: 4 –13 weeks) compared with 13 weeks (IQR: 8.3–21 weeks) for NICU infants.
Table 6 shows the descriptive statistics of age at iden-tification of hearing loss by degrees of hearing loss. Tukey B test indicated that there were no significant differences in identification age between the hearing loss
groups (F[2,130]⫽.046;P⫽.955).
Age at Enrollment in Early Support Programs
Median age for referral to education services, which in the United Kingdom provide the most common source of early support programs for families, was 10 weeks (IQR: 5–19 weeks).
Table 7 shows the age of enrollment to early support programs by degree of hearing loss. Tukey B tests indi-cated that there were no significant differences in age
between the groups (F[2,138]⫽1.039;P⫽.357).
Age at Hearing Aid Fitting
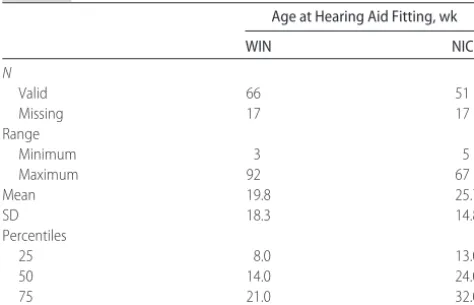
Median age at hearing aid fitting was 16 weeks, with the median age for WIN infants being 14 weeks (IQR: 8 –21 weeks) compared with 24 weeks (IQR: 13–32 weeks) for NICU infants.
The median delay from identification of hearing loss to hearing aid fitting was 5 weeks.
Table 8 shows the age of hearing aid fitting by degree of hearing loss. Tukey B tests indicated that there was a
significant difference between the groups (F[2,130] ⫽
8.667; P ⬍ .001); infants with moderate hearing loss
were fitted with hearing aids significantly later and fall
into a separate subset for␣⫽.05.
In 15 cases (9.9% of the cohort), the decision was
TABLE 4 Descriptive Statistics for Age at First Audiologic Assessment
Age at First Audiologic Assessment, wk
WIN NICU
N
Valid 77 66
Missing 5 4
Range
Minimum 0 1
Maximum 16 31
Mean 4.7 10.8
SD 3.0 7.3
Percentiles
25 3.0 4.5
50 4.0 9.0
75 5.8 17.0
TABLE 5 Descriptive Statistics for Age at Identification of Hearing Loss (separately for WIN and NICU population)
Age at First Identification of Hearing Loss, wk
WIN NICU
N
Valid 83 68
Missing 0 0
Range
Minimum 1 1
Maximum 62 56
Mean 11.7 16.0
SD 3.0 10.7
Percentiles
25 4.0 8.3
50 7.0 13.0
75 13.0 21.0
TABLE 6 Details of Reasons for Delay of the First Audiologic Follow-up Assessment (WIN Population)
Case No.
Age at the First Audiologic Follow-up
Assessment, wk
Explanation for the Delay
12 8 Service-related delay (long waiting time)
31 15 Missed the appointment (reason
unknown)
126 12 Nonresident; administrative difficulties
157 16 Bereavement in the family
172 10 Service-related delay (long waiting time)
185 12 Nonresident
233 11 Service-related delay (long waiting time)
242 13 Administrative difficulties
TABLE 7 Descriptive Statistics for Age Referral to Early Support Program
Age at Referral in Early Support Program, wk
WIN NICU
N
Valid 79 61
Missing 3 7
Range
Minimum 1 1
Maximum 123 56
Mean 7.0 17.5
SD 17.4 12.6
Percentiles
25 4.0 8.5
50 7.0 14.0
made not to fit hearing aids by the time of reporting: 7 moderate, 2 severe, and 6 profound hearing losses. For all these cases, the decision was made on the basis of parental choice.
Figure 1 presents the cumulative distributions for the 4 outcome measures used in these analyses: age at first follow-up appointment, age at identification of hearing loss, age at enrollment in early support program, and age of hearing aid fitting.
DISCUSSION
Median age at the first audiologic follow-up for infants subsequently identified as having a bilateral hearing loss was 5 weeks of chronologic age. Infants from the WIN tended to be followed up earlier. Infants from the NICU are often too ill and may have serious health problems that take immediate priority over possible hearing prob-lems. Infants from the NICU who will eventually be identified with profound hearing loss are followed up significantly later than infants who have lesser degrees of hearing loss, probably because these infants are most severely ill.
The reasons for exceptional delays to follow-up were different in WIN infants and NICU infants. In NICU
infants, these were related to the infant’s health and long hospitalization. In WIN infants, the reasons were service-related, mainly resulting from long waiting times for audiologic assessments and administrative slipups.
The newborn screening program first phase sites identified and informed the evaluation team of 169 in-fants with bilateral permanent hearing loss between their starting date (staggered from December 2001 to September 2002) and January 1, 2004. The yield for the period was 1.0 per 1000 infants screened, which is close to expected figures based on prevalence data (eg, 1.12
per 1000 from Fortnum and Davis5).
It is important to emphasize that the yield figure is significantly lower than demonstrated by most Northern American programs because the target case for the new-born hearing screening in England does not include
unilateral or mild hearing loss. The report by Davis et al9
concluded that there was a strong case to be made for a universal newborn hearing screen to identify bilateral
permanent hearing loss ofⱖ40-dB hearing loss. Davis et
al9argued that although there was no denying the effects
of mild or unilateral permanent congenital hearing loss on speech perception in noisy backgrounds and on var-ious aspects of educational achievement, mild or unilat-eral hearing loss did not constitute serious public health hazard; there was no unequivocal evidence of effective-ness, particularly cost-effectiveeffective-ness, of screening for these conditions at birth; and there was no robust evi-dence about whether intervention would be effective. Unilateral test/screen fails are retested and referred to increase the sensitivity of the screen, not to specifically identify unilateral hearing loss. As expected, some cases of unilateral hearing loss as well as mild hearing loss are nevertheless detected by the screen. Evidence-based guidelines for management of unilateral and mild hear-ing loss are urgently needed in England.
The distribution of degree of hearing loss is somewhat
different from previous studies. Fortnum and Davis5
found that moderate hearing loss was more prevalent than severe and profound hearing loss put together. In the present cohort, profound hearing loss was more common than expected. It should be noted that the category of hearing loss for any particular child was determined in the early stages of the assessment/diag-nostic procedures, and that these may change as more accurate information emerges. On the other hand, if preferred practice guidelines for assessment are followed
properly (see www.nhsp.info),12 then accurate
assess-ment should be possible by 6 months of age in most cases; furthermore, in all cases, the clinicians maintained the reported degree of hearing loss when they fitted the hearing aids, suggesting a high degree of certainty about degree of loss. Thus, the reasons for the somewhat dif-ferent distribution of degrees of hearing loss in the cur-rent cohort are unclear; assessment difficulties for mod-erate hearing loss may play a part, but a secular trend for
TABLE 8 Descriptive Statistics for Hearing Aid Fitting
Age at Hearing Aid Fitting, wk
WIN NICU
N
Valid 66 51
Missing 17 17
Range
Minimum 3 5
Maximum 92 67
Mean 19.8 25.7
SD 18.3 14.8
Percentiles
25 8.0 13.0
50 14.0 24.0
75 21.0 32.0
FIGURE 1
an increase in the proportion of profound hearing losses (eg, in the increasing population of NICU infants) is also a real possibility. Such a possibility will be confirmed, or not, as the newborn screening program rolls out and the number of true cases increases.
Not surprisingly, sensorineural hearing loss was the most common type of hearing loss. Approximately 10% of the cohort of true cases were identified with auditory
neuropathy; this is in line with other studies.13,14 All
infants identified with auditory neuropathy were from the NICU population as a result of the protocol adopted for NICU infants; any cases from the WIN population (thought to be a much lower prevalence) will have to emerge over time.
Risk factors for permanent congenital hearing loss are well established. The 3 major risk factors are (1) a history
of admission to NICU for⬎48 hours, (2) a family history
of early childhood permanent deafness, and (3) a cranio-facial anomaly (eg, cleft palate) associated with
perma-nent hearing loss.5,15 Ninety-one of the 169 true cases
(54%) had ⱖ1 of these risk factors, which is similar to
published estimates.5,15 The proportion of high-risk
in-fants of all permanent bilateral hearing loss cases is in
line with Davis and Wood15 and Fortnum and Davis5;
approximately 60% of all congenitally impaired children
had ⱖ1 risk factors. However, there may be a shift
toward the increase in the proportion of NICU infants, with 44% in this cohort as opposed to 29% found in both previously mentioned studies. The proportion with a family history of permanent childhood deafness was just 19%, which may reflect the complexity of history-taking at such an early stage. Craniofacial anomalies were present in 9%, which is between the 4% reported
by Davis and Wood15and the 12% reported by Fortnum
and Davis.5The high proportion of cases with risk factors
led, in the early 1990s, to the widespread introduction of “at-risk” newborn screening in which attempts were made to screen all those infants (just under 10% of the birth cohort) with risk factors. However, in practice, as a
result of the difficulty obtaining accurate risk status,6,16
the proportion of the target population identified by
at-risk screening was rarely ⬎40%. Therefore, it is
un-safe to assume that all these 91 infants with risk indica-tors identified with hearing loss would have been found through targeted newborn hearing screening.
The median age of identification for those screened neonatally has been shown in research studies to be of
the order of 2 months.16–18 The findings from this
eval-uation of the first phase of a population-based national program are in line with that; the median age of identi-fication was 10 weeks. Although this applies only to the limited cohort and does not take into consideration po-tential screen false-negatives or infants who missed the screen, compared with the situation before the introduc-tion of screening, when the median age at identificaintroduc-tion
of bilateral permanent hearing loss in the United
King-dom was 26 months,5this is a massive improvement.
Importantly, given that intervention has been argued to be beneficial for degrees of hearing loss down to at
least moderate levels,9age at identification was
indepen-dent of the degree of hearing loss. This was not the case before the introduction of NHSPs.
Before the introduction of newborn hearing screen-ing, NICU infants with hearing loss were identified
ear-lier.9In the current evaluation, infants from the healthy
infant population were identified significantly earlier than those from NICU. When there were delays in iden-tification, these were often the result of assessment and service difficulties in the well-infant population, whereas in NICU infants, the delay was more likely to be associated with the health of the infant. Also, it is im-portant to point out in the present analysis, chronologic ages were compared instead of corrected ages and that is likely to add to the difference between the outcome measures in the 2 nursery types.
Median age of enrollment in the early support pro-gram is of course strongly correlated with the age of identification of hearing loss, because according to the
quality standards,17all children who are identified with
bilateral moderate or greater hearing loss should be re-ported to education services within 1 working day of identification.
The median age at hearing aid fitting of 16 weeks was
similar to that reported elsewhere.18–20 This is a
signifi-cant improvement compared with the average age of 32 months in the United Kingdom before the
implementa-tion of newborn hearing screening.5 Of course, a few
screen false-negatives may yet be identified, and not all subjects identified had hearing aids fitted; therefore, this median age may therefore change, but it is unlikely to be by a significant amount.
For the whole cohort, age at hearing aid fitting is the first event in which degree of hearing loss has an effect; infants with moderate hearing loss are fitted with hear-ing aids significantly later than those with severe or profound hearing loss; possible reasons are parental ret-icence (and the exercise of parental choice) in the light of some auditory responsiveness and assessment uncer-tainty. For NICU infants, those with profound (as well as moderate) hearing loss are fitted significantly later than those with severe hearing loss, presumably as a result of other difficulties.
CONCLUSIONS
per-manent hearing loss as early as possible. Analyses of 169 cases reported from 23 first phase sites and based on 170 000 infants screened shows that the age markers chosen all occurred within the first few weeks and months of age. The descriptive statistics of the cases suggested that there are unlikely to be significant num-bers of false-negatives or missed cases, and that in the main the profile of the cases was as expected; the pos-sibility that the proportion of subjects with profound hearing loss is on the increase as a result of develop-ments in the NICU practice merits additional investiga-tion. A key feature of the NHSP program in England is the extent of planned and centrally funded implemen-tation and “top-down” direction (involving, eg, a na-tional IT screening management system, nana-tional train-ing for screeners, preferred practice guidelines, and so on). It is highly likely that the positive outcomes re-ported here are closely linked to this public health ap-proach to population-based screening.
ACKNOWLEDGMENTS
This work was undertaken by the evaluation team for the implementation of newborn hearing screening pro-gram in England; the evaluation was funded by the Department of Health.
We thank Professor Adrian Davis and his team, as well as everybody in the local screening teams from all 23 first-phase newborn hearing screening program sites, particularly the staff from pediatric audiology services.
REFERENCES
1. Fortnum HM, Summerfield AQ, Marshall DH, Davis AC, Bam-ford JM. Prevalence of permanent childhood hearing impair-ment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study.BMJ.2001;323:536 –539
2. Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Language of early- and later-identified children with hearing loss. Pedi-atrics.1998;102:1161–1171
3. Thompson DC, McPhillips H, Davis R, Lieu T, Homer C, Hel-fand M. Universal Newborn Hearing Screening. Summary of evidence.JAMA.2001;286:2000 –2010
4. Hyde ML. Evidence-based practice, ethics and EHDI program
quality. In: Seewald RC, Bamford J, eds.A Sound Foundation Through Early Amplification(Proceedings of the 3rd International Pediatric Conference). Basel, Switzerland: Phonak AG; 2005 5. Fortnum H, Davis A. Epidemiology of permanent hearing
im-pairment in Trent region, 1985–1993.Br J Audiol.1997;31:409 – 446
6. Vohr BR, Carty LM, Moore PE, Letourneau K. The Rhode Island hearing assessment program: experience with statewide hearing screening (1993–1996).J Pediatr.1998;133:353–357 7. Parving A, Hauch AM, Christensen B. Hearing loss in children:
epidemiology, age at identification and causes through 30 years [in Danish].Ugeskr Laeger.2003;165:574 –579
8. Deben K, Janssens de Varebeke S, Cox T, Van de Heyning P. Epidemiology of hearing impairment at three Flemish Insti-tutes for Deaf and Speech Defective Children. Int J Pediatr Otorhinolaryngol.2003;67:969 –975
9. Davis A, Bamford J, Wilson I, Ramkalawan T, Forsaw M, Wright S. A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
Health Technol Assess.1997;1:i–iv, 1–176.
10. Wilson JMG, Junger G. Principles and Practice of Screening for Disease. Geneva, Switzerland: World Health Organization; 1968 11. Davis A, Hind S. The newborn hearing screening programme in England.Int J Pediatr Otorhinolaryngol.2003;67:S193–196 12. Newborn hearing screening programme. Audiology protocols
(10 screens). Available at: www.nhsp.info/cms.php?folder⫽21. Accessed February 4, 2005
13. Rance G, Beer DE, Cone-Wesson B, et al. Clinical findings for a group of infants and young children with auditory neurop-athy.Ear Hear.1999;20:238 –252
14. Sininger YS. Identification of auditory neuropathy in infants and children.Semin Hear.2002;23:193–200
15. Davis A, Wood, S. The epidemiology of childhood hearing impairment: factors relevant to planning services.Br J Audiol.
1992;26:77–90
16. Watkin P. Neonatal otoacoustic emission screening and the identification of deafness.Arch Dis Child.1996;74:16 –25 17. Quality Standards in Paediatric Audiology.Vol IV. London, United
Kingdom: National Deaf Children’s Society; 2000
18. Harrison M, Roush J, Wallace J. Trends in age of identification and intervention in infants with hearing loss.Ear Hear.2003; 24:89 –95
19. Dalzell L, Orlando M, MacDonald M, et al. The New York State universal newborn hearing screening demonstration project: ages of hearing loss identification, hearing aid fitting, and enrollment in early intervention.Ear Hear.2000;21:118 –130 20. Yoshinaga-Itano C. Early intervention after universal neonatal
DOI: 10.1542/peds.2005-1064
2006;117;e887
Pediatrics
Kai Uus and John Bamford
of Interventions and Profile of Cases
Effectiveness of Population-Based Newborn Hearing Screening in England: Ages
Services
Updated Information &
http://pediatrics.aappublications.org/content/117/5/e887 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/117/5/e887#BIBL This article cites 16 articles, 2 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
orders_sub
http://www.aappublications.org/cgi/collection/ear_nose_-_throat_dis Ear, Nose & Throat Disorders
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2005-1064
2006;117;e887
Pediatrics
Kai Uus and John Bamford
of Interventions and Profile of Cases
Effectiveness of Population-Based Newborn Hearing Screening in England: Ages
http://pediatrics.aappublications.org/content/117/5/e887
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.