www.wjpr.net Vol 4, Issue 09, 2015.
298
DETERMINATION OF DRUG RESISTANT STRAINS CAUSING
URINARY TRACT INFECTIONS WITH MIC AND DISK DIFFUSION
METHODS
Afsaneh Karami*1, saideh Mazloom Zadeh2, Ala Rastin3, mehdi ojagh faghihi4, Afroozeh Karami5
1
Department of Infectious Disease, Zanjan University of Medical Sciences, Zanjan, IR Iran.
2.
Epidemiology and Biostatistics Department, Zanjan University of Medical Sciences,
Zanjan, IR Iran.
3
Shahid Beheshti Hospital. Zanjan University of Medical Sciences, Zanjan, IR Iran.
4
Vali-e-asr Hospital, zanjan University of Medical Sciences, Zanjan, IR Iran.
5
Zanjan University of Medical Sciences, Zanjan, IR Iran.
ABSTRACT
Introduction: Urinary tract infection (UTI) is one of the most prevalent bacterial infections. Wide ranges of antibiotics are used for
treatment of UTI. Studies revealed that the antimicrobial therapies are
not effective many times and excessive use of antibiotics could result
in development of multidrug resistance organisms. Determination of
causative strains for infection and especially the pattern of antibiotic
resistance in each area are essential to find a proper antibiotic for the
first-line therapy and consequently preventing from more drug
resistance by prescribing the better drugs. Materials and Methods:
This cross sectional study was performed from 2011 to 2012 on the
organisms collected from urine culture of UTI patients who were
hospitalized at Vali-ye-Asr Hospital in Zanjan, Iran. To define the type of strains the
organisms were cultured in differential medium and the type of strain was determined by
adding anti serum and using tables for the type of strains. After determination of the strains of
each organism for collected urine cultures, the drug resistance was assessed using MIC
(Minimum Inhibitory Concentration) and disc diffusion methods. Results: among 223
patients, 58.7% were female, and their mean age was 64 ± 0.18 years old. The most common
organisms were Escherchia coli (44.8%) and streptococcus (15.7%). The disk diffusion test
Volume 4, Issue 9, 298-310. Research Article ISSN 2277– 7105
Article Received on 30 June 2015,
Revised on 24 July 2015, Accepted on 18 Aug 2015
*Correspondence for Author
Dr. Afsaneh Karami
Department of Infectious Disease, Zanjan
University of Medical Sciences, Zanjan, IR Iran.
www.wjpr.net Vol 4, Issue 09, 2015.
299
showed highest resistance of vancomycin (83.3%), Nalidixic Acid (83%) and Ampicillin
(80.7%). With the MIC method highest resistance was from Ampicillin, cephalexine,
co-tromoxazole (each one with 92.4% resistancy). In disk diffusion method the most common
Resistancy were in patients over 60 years old , and in MIC method resistancy was more
common in 41-60 years old patients with vancomycin , cefixime , Gentamicin and
co-Amoxiclave. In male patients Resistancy with ceftriaxone and Gentamicine and in female
with vancomycin and co-Amoxiclave were the heighest. With underlyind diseases resistancy
to co-trimoxazole, Ampicillin, co-Amoxiclave, cefixime, cephalexin, ceftriaxone,
Nitrofurantoin, Gentamicin and ciprofloxacin was heighest, and in MIC method to
ciprofloxacin and co-trimoxazole was more common. And the differences were statistically
significant. The highest sensitivity of disk method was from nitrofurantoin with 84.7%
sensitivity, and the highest specitivity was from nalidixic Acid (89.2%). The Correlation
between MIC and disk diffusion method for diagnosis of nitrofurantoin, ofloxacin, nalidixic
acid resistancy was observed. Conclusions: Because of high sensitivity of Nitrofurantoin,
Imipenem and Gentamicin, with disk diffusion and MIC methods, it seems that these drugs
are preffered for treatment and prevention of Urinary tract infections. As Gentamicin,
cephalexin and co-trimoxazole showed high resistancy, it’s recommended to avoid using of
them for those infections.
KEYWORDS: Microbial Sensitivity Tests; Disk Diffusion Antimicrobial Tests; Urinary Tract Infections; Organism, Microbial Sensitivity Tests; Drug Resistance, Bacterial
1. INTRODUCTION
Urinary tract infection (UTI) which specified as urinary system infection is one of the most
prevalent bacterial infections.[1] It is the second common infection after respiratory
infections,[2] Both the lower and upper urinary tracts can be involved by UTI.[1] Some
different conditions are considered for UTI including UTI, Asymptomatic bacteriuria,
Symptomatic UTI, Uncomplicated UTI, Complicated UTI, Recurrent UTI and Urosepsis.[3]
Symptomatic UTI is determined by the specific symptoms of UTI with a significant
bacteriuria with a quantitative count of ≥105
CFU/ml in a urine sample,[4,5] The presence of
bacteria in the urine without the symptoms of UTI is considered as
Asymptomaticbacreriuria,[4] Uncomplicated UTI is distinguished by a symptomatic bladder
www.wjpr.net Vol 4, Issue 09, 2015.
300
is due to the structural and functional disorders such as organ transplantation, diabetes or
renal failure are considered as complicated UTI.[6, 7]
Almost 150 million individuals throughout the world experience the UTI at least once during
their lifetime.[8] The prevalence of UTI in United States is about more than eight million per
year and almost all of the patients with UTI undergone antibiotic therapy and a restricted
numbers of them should be hospitalized.[9, 10]
In all age groups the prevalence of UTI are higher among women than men with the ratio of 8
women per one man.[11] By age 24 one out of three women will face with UTI and 50% of
women experience UTI during their life,[10] It was shown that the rate of UTI incidence is
higher in elderly men and women especially after the age of 85,[12, 13] In addition, UTI is one
of the usual diseases among children with the prevalence of 2-8% during childhood.[14]
The Escherichia coli (E coli)is the main cause of the UTI. After that Enterobacteraciae
including Klebsiella, Providentia and Proteus mirabilis species are at the second place.
Methicillinresistant Staphylococcus aureus and Enterococcus as gram positive organisms are
of little importance.[15, 16]
Wide ranges of antibiotics are used for treatment of UTI. Amoxicillin, ampicillin, and
sulfonamides are not proper options for UTI treatment since the E coli is resistance to
them.[17-19] Amoxicillin/clavulanic and nitrofurantoin are still effective although
nitrofurantoin shouldn’t prescribe for patients with renal failure.[20] According to
International Clinical Practice Guidelines for the Treatment of Acute Cystitis, for the
treatment of uncomplicated UTIs treating with trimethoprim-sulfamethoxazole (TMP-SMX)
for three days and nitrofurantoin for five days are suggested as the first-line therapy.[21, 22] If
first-line therapies are not possible beta-lactams, such as amoxicillin/clavulanic acid and
cefaclor for 3-7 days is recommended.[19, 21] In a study by Falagas et al., it was revealed that
fosfomycintrometamol is another effective choice for treatment of UTIs. However, the
previous therapies are a little more effective,[23] Fluoroquinoloneis one of the most common
antibiotics for UTI, but resistance to these antibiotics is high and they shouldbe used after
performing the sensitivity test.[15] TMP-SMX, fluoroquinolones and nitrofurantoin are useful
www.wjpr.net Vol 4, Issue 09, 2015.
301
Many of the antimicrobial therapies are not effective sometimes and excessive useof
antibiotics could result in development of multidrug resistance organisms. Since due to acute
symptoms of UTI the antibiotic therapy will be started before receiving the result of urine
culture and antibiogram, determination of causative strains for infection and especially the
pattern of antibiotic resistance in each area is essential to find a proper antibiotic for the
first-line therapy and consequently preventing from more drug resistance by prescribing the better
drugs.
2. MATERIALS AND METHODS
This is a cross sectional study and was performed from 2011 to 2012. Organisms were
collected from urine culture of patients who diagnosed with UTI and hospitalized at
Vali-ye-Asr Hospital in Zanjan, Iran. The clinical symptoms of patients were fever, chills, suprapubic
tenderness, frequent urination, dysuria and gastrointestinal symptoms such as vomiting and
diarrhea, sepsis and septic shockandthe diagnosis was confirmed by an infectious disease
specialists. The urine culture was performed by midstream clean catch method. Positive result
for women was determined by equal to or more than 102 organisms and for men by equal to
or more than 103 organisms. After determination of the strains of each organism for collected
urine cultures, the drug resistance was assessed using disc diffusion and MIC (Minimum
Inhibitory Concentration) methods. Antimicrobial susceptibility was evaluated for 13
antibiotics including Ciprofloxacin, Nitrofurantoin, Ampicillin, Ofloxacin, Cotrimoxazole,
Cephalexin, Gentamicin, Ceftriaxone, Nalidixic acid, Imipenem, Ceftizoxime, Co-amoxiclav
and Vancomycin.
To define the type of strains the organisms were cultured in differential medium and the type
of strain was determined by adding anti serum and using tables for the type of strains.
Macrotube method was used for MIC. First of all the stock solution was prepared which
required the antibiotic weight (mg) [Volume (ml) × concentration (µg/ml)/Assay potency
(µg/mg)] and the volume of diluent (ml) [Weight (mg) × Assay potency)/Concentration].
To prepare the microbial suspension from isolated colonies ofmedium with 18-24 h
incubation, they directlyinoculated to liquid Muller Hilton to provide a turbidity similar to 0.5
McFarland (to prepare the McFarland 0.5 mL of barium chloride dihydrate solution [Bacl2 &
2H20] was added to 99.5 mL of 1% Sulfuric acid and the OD of the solution was assessed at
www.wjpr.net Vol 4, Issue 09, 2015.
302
of antibiotics was added to the tubes with screw caps and 1 mL of microbial suspension was
included. Thus, by doubling the volume, the final concentration of the antibiotic in each tube
is half of the initial calculated concentration. Then thetubes wereincubatedfor16-20hoursat
35°C moist and at the end the resultswere read. The read numbers of MIC were reported
according to the Clinical and Laboratory Standards Association (CLSI) guideline. Drug
resistance was calculated using the disk diffusion method too. A questionnaire was prepared
and the demographic futures of the patients and the results of MIC and antibiogramwith disc
were recorded in it.
2.1. STATISTICAL ANALYSIS
Data were analyzed using Spss version 18. Chi square test, frequency distribution tables and
measures of central tendency and dispersion were used to analyze the data.
3. RESULTS
From positive urine cultures, 224 cases which was confirmed of urinary tract infection were
selected. Bacterial resistance was done for all samples with two disk diffusion and MIC test
methods. The percent of female and male gender was 58.7:41.3 and the age range was about
64 ± 0.18. The most isolated organism was E. coli (44.8%) and Streptococcus (15.7%).
3.1. GENDER
Antibiotic susceptibility test has been performed on all the samples and result was different
based on the gender of patients. Disk diffusion test result can be seen in Table 1 and MIC
result are available in Table 2. In disk diffusion method most resistance to ceftriaxone and
gentamicin were seen in male subjects. Also in MIC method this resistance were belonged to
female subjects to vancomycin and co-amoxiclav antibiotic.
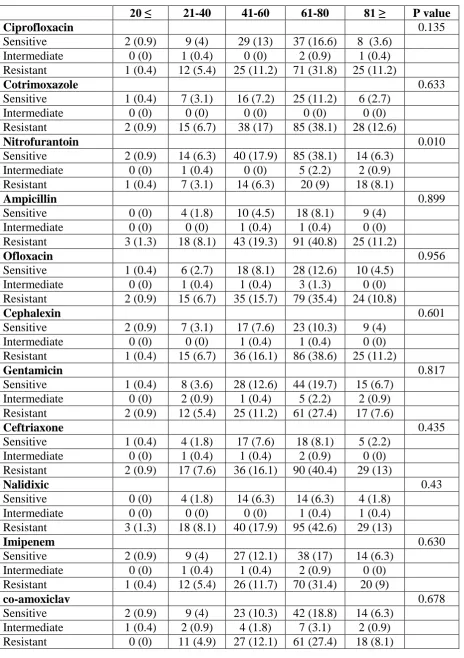
3.2. AGE
The age range of patients was about 64.8 ± 0.18 (Min = 19, Max = 102). The result of the
MIC and disk diffusion test on samples based on age parameter of patients has been shown in
Tables 3 and 4. In disk diffusion method most drug resistance were found in people over 60
years old and in MIC, the greatest resistance to were seen at the age of 60-41 years to
www.wjpr.net Vol 4, Issue 09, 2015.
[image:6.595.69.534.108.766.2]303 Table 1. Frequency of Antibiotic Resistance in the Disk Diffusion Method based on Age Parameter
20 ≤ 21-40 41-60 61-80 81 ≥ P value
Ciprofloxacin 0.135
Sensitive 2 (0.9) 9 (4) 29 (13) 37 (16.6) 8 (3.6)
Intermediate 0 (0) 1 (0.4) 0 (0) 2 (0.9) 1 (0.4)
Resistant 1 (0.4) 12 (5.4) 25 (11.2) 71 (31.8) 25 (11.2)
Cotrimoxazole 0.633
Sensitive 1 (0.4) 7 (3.1) 16 (7.2) 25 (11.2) 6 (2.7)
Intermediate 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Resistant 2 (0.9) 15 (6.7) 38 (17) 85 (38.1) 28 (12.6)
Nitrofurantoin 0.010
Sensitive 2 (0.9) 14 (6.3) 40 (17.9) 85 (38.1) 14 (6.3)
Intermediate 0 (0) 1 (0.4) 0 (0) 5 (2.2) 2 (0.9)
Resistant 1 (0.4) 7 (3.1) 14 (6.3) 20 (9) 18 (8.1)
Ampicillin 0.899
Sensitive 0 (0) 4 (1.8) 10 (4.5) 18 (8.1) 9 (4)
Intermediate 0 (0) 0 (0) 1 (0.4) 1 (0.4) 0 (0)
Resistant 3 (1.3) 18 (8.1) 43 (19.3) 91 (40.8) 25 (11.2)
Ofloxacin 0.956
Sensitive 1 (0.4) 6 (2.7) 18 (8.1) 28 (12.6) 10 (4.5)
Intermediate 0 (0) 1 (0.4) 1 (0.4) 3 (1.3) 0 (0)
Resistant 2 (0.9) 15 (6.7) 35 (15.7) 79 (35.4) 24 (10.8)
Cephalexin 0.601
Sensitive 2 (0.9) 7 (3.1) 17 (7.6) 23 (10.3) 9 (4)
Intermediate 0 (0) 0 (0) 1 (0.4) 1 (0.4) 0 (0)
Resistant 1 (0.4) 15 (6.7) 36 (16.1) 86 (38.6) 25 (11.2)
Gentamicin 0.817
Sensitive 1 (0.4) 8 (3.6) 28 (12.6) 44 (19.7) 15 (6.7)
Intermediate 0 (0) 2 (0.9) 1 (0.4) 5 (2.2) 2 (0.9)
Resistant 2 (0.9) 12 (5.4) 25 (11.2) 61 (27.4) 17 (7.6)
Ceftriaxone 0.435
Sensitive 1 (0.4) 4 (1.8) 17 (7.6) 18 (8.1) 5 (2.2)
Intermediate 0 (0) 1 (0.4) 1 (0.4) 2 (0.9) 0 (0)
Resistant 2 (0.9) 17 (7.6) 36 (16.1) 90 (40.4) 29 (13)
Nalidixic 0.43
Sensitive 0 (0) 4 (1.8) 14 (6.3) 14 (6.3) 4 (1.8)
Intermediate 0 (0) 0 (0) 0 (0) 1 (0.4) 1 (0.4)
Resistant 3 (1.3) 18 (8.1) 40 (17.9) 95 (42.6) 29 (13)
Imipenem 0.630
Sensitive 2 (0.9) 9 (4) 27 (12.1) 38 (17) 14 (6.3)
Intermediate 0 (0) 1 (0.4) 1 (0.4) 2 (0.9) 0 (0)
Resistant 1 (0.4) 12 (5.4) 26 (11.7) 70 (31.4) 20 (9)
co-amoxiclav 0.678
Sensitive 2 (0.9) 9 (4) 23 (10.3) 42 (18.8) 14 (6.3)
Intermediate 1 (0.4) 2 (0.9) 4 (1.8) 7 (3.1) 2 (0.9)
www.wjpr.net Vol 4, Issue 09, 2015.
304
Cefixime 0.803
Sensitive 2 (0.9) 5 (2.2) 15 (6.7) 13 (5.8) 8 (6.3)
Intermediate 0 (0) 0 (0) 0 (0) 3 (1.3) 0 (0)
Resistant 1 (0.4) 17 (7.6) 39 (17.5) 94 (42.2) 26 (11.7)
Vancomycin 0.401
Sensitive 1 (0.4) 6 (2.7) 7 (3.1) 11 (4.9) 4 (1.8)
Intermediate 0 (0) 0 (0) 2 (0.9) 5 (2.2) 0 (0)
Resistant 2 (0.9) 16 (7.2) 45 (20.2) 94 (42.2) 30 (13.5)
Data are presented as No. (%)
3.3. Having a History of Disease or Previous Use of Antibiotics
In patients with history of a disease drug resistance were seen to cotrimoxazole, ampicillin,
co-amoxiclav, cefixime, cephalexin, ceftriaxone, nitrofurantoin, gentamicin and ciprofloxacin
in in disc diffusion method and to cotrimoxazole and ciprofloxacin in MIC method. In
patients with a history of antibiotic use difference was only significant for ciprofloxacin in
MIC method.
As the result of this study the drug sensitivity of each organism that achieved with MIC
www.wjpr.net Vol 4, Issue 09, 2015.
[image:8.792.0.792.92.241.2]305 Table 3. Drug Sensitivity for Each Organism in disk diffusion Method
Organism ciprofloxacin Ofloxacin Nalidixic acid Ceftriaxone Cefixime Cephalexin Co-amoxiclav Ampicillin Imipenem Cotrimoxazole Nitrofurantoin Gentamicin Vancomycin
S R S R S R S R S R S R S R S R S R S R S R S R S R
Escherchia
coli (35.4)53
64 (64.6) 28 (28.3) 69 (69.7)
15(15.2) 84 (84.8) 25 (25.3) 74 (74.7) 22 (22.2) 57 (57.8) 27 (27.3) 72 (72.7) 43 (43.4) 56 (56.6) 13 (13.1) 86 (86.8) 40 (40.6) 59 (59.4) 23 (23.2 76 (76.8) 76 (76.8) 23 (23.2) 49 (49.5) 50 (50.5)
2 (2) 97 (98)
streptococcus 8 (3.6) 27 (12.1) 6 (17.1) 29 (82.9)
5 (14.3) 30 (85.7) 2 (5.7) 33 (94.3) 2 (5.7) 33 (94.3)
7 (20) 28 (80) 19 (54.3) 16 (45.7) 16 (45.7) 19 (53.4)
7 (20) 28 (80) 6 (17.1) 29 (82.9) 24 (68.6) 11 (31 .4) 5 (14.3) 30 (85.7) 12 (34.3) 23 (65.7)
staphylococcus 10 (47.6) 11 (52.4) 7 (33.3) 14 (66.7)
3 (14.3) 18 (85.7) 1 (4.8) 20 (95.2) 6 (28.6) 15 (71.4) 10 (47.6) 11 (52.4) 12 (57.1) 9 (42.9) 5 (23.8) 16 (76.2) 9 (42.9) 12 (57.1) 7 (33.3) 14 (66.7) 14 (66.7) 7 (33.3) 10 (47.6) 11 (52.4) 13 (61.9) 7 (33.3)
Seratia 6
(36.4) 7 (63.6) 2 (18.2) 9 (81.8)
3 (27.3) 8 (72.7) 4 (36.4) 7 (63.6) 2 (18.2) 9 (81.8) 2 (18.2) 9 (81.8) 3 (27.3) 8 (72.7) 1 (9.1) 10 (90.9) 5 (45.5) 6 (54.5) 5 (54.5) 6 (45.5) 9 (81.8) 2 (18.2) 7 (63.6) 6 (36.4)
0 (0) 11 (100)
pseudomonas 8 (61.5) 5 (38.5) 7 (53.8) 6 (46.2)
0 (0) 13
(5.8) 2 (15.4) 11 (84.6) 2 (15.4) 11 (84.6) 2 (15.4) 11 (84.6) 1 (7.7) 12 (92.3)
0 (0) 13 (100)
8 (61.5)
4 (30.8)
0 (0) 13 (100) 1 (7.7) 12 (92.3) 6 (46.2) 7 (53.8)
0 (0) 13 (100)
klebsiella 6 (42.9) 8 (57.1) 4 (28.6) 10 (71.4)
4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 6 (42.9) 8 (57.1) 2 (14.3) 12 (85.7)
7 (50) 7 (50) 4 (28.6) 10 (71.4) 10 (71.4) 3 (21.4)
7 (50) 7 (50) 0 (0) 14 (100)
Others* 11
(42.3) 15 (57.7) 6 (23,1) 20 (76.9)
4 (15.3) 22 (84.7) 3 (11.5) 23 (88.5) 3 (11.5) 23 (88.5) 2 ( 11.6) 24 ( 88.4) 3 (11.5) 23 (88.5) 1 (3.8) 25 (98.2) 8 (30.8) 18 (69.2) 6 ( 23.1) 20 (76.9) 17 (82.3) 9 (17.7) 6 (23,1) 20 (76.9) 1 (3.8) 25 (96.2)
*Includes Edwardsiella, Acinetobacter, Citrobacter, Enterobacter, Mvrganla, Providencia, Proteus, and yeast
Data are presented as No. (%)
Table 4.Drug Sensitivity for Each Organism in MIC Method
Organism ciprofloxacin Ofloxacin Nalidixic acid Ceftriaxone Cefixime Cephalexin Co-amoxiclav Ampicillin Imipenem Cotrimoxazole Nitrofurantoin Gentamicin Vancomycin
S R S R S R S R S R S R S R S R S R S R S R S R S R
Escherchi a coli 11 (11.1) 88 (88.9) 19 (19.2) 80 (80.8) 10 (10.1) 89 (89.9) 9 (9.1) 90 (90.9)
3 (3) 96 (97)
1 (1) 98 (99)
10 (10.1)
89 (90.9)
2 (2) 97 (98) 16 (16.1)
83 (83.9)
2 (2) 97 (98) 65 (65.7) 34 (34.3) 27 (27.3) 72 (82.7)
0 (0) 99 (100) streptococ cus 12 (34.3) 23 (65.7) 15 (42.9) 20 (57.1) 14 (40) 21 (60) 11 (31.4) 24 (68.8) 11 (31.4) 23 (65.7) 6 (17.1)
) (82.9)92 23 (65.7) 12 (34.3) 01 (28.6)
) )(71.4)92 14 (40) 21 (60) 9 (25.7) 96 (74.3) ) 27 (22.6) 8 (12.4) 09 (10.5) ) 23 (17.6) 24 (68.6) 11 (31.4) staphyloc occus 9 (42.9) 13 (57.1) 7 (33.3) 14 (66.7)
8 (38) 13 (62) 5 (23.8) 16 (76.2) 2 (9.5) 19 (88.5) 10 (47.6) 11 (52.4) 12 (57.1) 9 (42.9) 5 (23.8) 16 (76.2) 9 (42.9) 12 (57.1) 7 (33.3) 14 (66.7) 14 (66.7) 7 (33.3) 10 (47.6) 11 (52.4) 13 (61.9) 8 (38.1)
Seratia 4 (36.4) 7 (63.6) 2 (18.2) 9 (81.8) 3 (27.3) 8 (72.7) 4 (36.4) 7 (63.6) 2 (18.2) 7 (63.6) 2 (18.2) 9 (81.8) 3 (27.3) 8 (72.7)
1 (9.1) 10 (90.9) 5 (54.5) 6 (45.5) 5 (54.5) 6 (45.5) 9 (81.8) 2 (18.2) 7 (63.6) 4 (36.4)
0 (0) 11 (100) pseudomo nas 8 (61.5) 5 (38.5) 7 (53.8) 6 (46.2)
0 (0) 13 (100) 2 (15.4) 11 (84.6) 2 (15.4) 11 (84.6) 2 (15.4) 11 (84.6) 1 (7.7) 12 (92.3)
0 (0) 13
(100) 8 (61.5)
4 (30.8)
0 (0) 13 (100) 1 (7.7) 12 (92.3) 6 (46.2) 7 (53.8)
0 (0) 13 (100)
klebsiella 6 (42.9) 8 (57.1) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 4 (28.6) 10 (71.4) 6 (42.9) 8 (57.1) 2 (14.3) 12 (85.7)
7 (50) 7 (50) 4 (28.6) 10 (71.4) 10 (71.4) 4 (28.6)
7 (50) 7 (50) 0 (0) 14 (100)
Others* 13
(50) 13 (50) 8 (30.7) 18 (69.3) 4 (15.3) 22 (84.7) 6 (23.1) 20 (76.9) 4 (15.3) 22 (84.7) 5 (19.2) 21 (80.8) 4 (15.3) 22 (84.7) 6 (23.1) 20 (76.9) 12 (46.1) 14 (53.9) 6 (23.1) 20 (76.9) 23 (88.4) 3 (11.6) 10 (38.4) 16 (61.6) 2 (7.7) 24 (92.3)
*Includes Edwardsiella, Acinetobacter, Citrobacter, Enterobacter, Mvrganla, Providencia, Proteus, and yeast
www.wjpr.net Vol 4, Issue 09, 2015.
306 4. DISCUSSION
The prevalence of urinary tract infection is more common in women and as the other studies and
implementation the same results can be seen at the present study.[26-18] In this study that
performed at Ahwaz, Iran, E. coli in women, and Pseudomonas in men was the most common
isolated organism. In a study performed in Hong Kong, the rate of resistance to ampicillin,
nalidixic acid, ciprofloxacin and trimethoprim-sulfamethoxazole in women over 51 years was
more than women 50-18 years old.[29] In another study in Brazil, the rate of resistance to
quinolones reported 25% in men and 9% in women.[30]
In a study performed in South America, enterococci and streptococci were the most common
isolated organisms in women (responsible for 5.2% and 2.8% of infections) and only 8 S.
saprophyticus was isolated.[31] The difference in the organism and drug resistance in both sexes
in other studies may be related to pervious disease and risk factors predisposing to infection and
different consumption patterns for antibiotics in different communities.
The age range of the patients participate in this study was 65.8 ± 0.18 and the most drug resistant
in MIC method were seen in patients over 60 years old but this resistance in MIC methods was in
41-60 years old and to vancomycin, cefixime, gentamicin and co-amoxiclav. In Andrade et al.
study the age range was 42 years,[31] In another study in Spain with the age range of 54.1 the
resistant to ciprofloxacin in patients younger than 40 years old was 6.7% and in patient older
than 60 years old was 33.9%.[32] Shaban et al. reported the 5% resistance to ciprofloxacin in
adults and 13% and 14% resistance to amikacin and co-amoxiclav respectively in men over 50
years old.[33] Regarding the increasing use of antibiotics with ageing result of the above studies
would be expected.
In present study 84.3% of the participants had a background of another disease and drug resistant
was more in such patients. In a study by Ladhani et al. the patients with renal problems had
62.5% more resistance in compare with patients without other disease.[34] A 5 years study in
England showed that resistant to trimethoprim has been increased from 24.1 to 31.6 in children
under 15 years old.[35]
In conclusion due to the high sensitivity of nitrofurantoin, gentamicin and imipenem, with disk
www.wjpr.net Vol 4, Issue 09, 2015.
307
tract infections. Since gentamicin, cephalexin and cotrimoxazole showed high resistance, it is
recommended that the use of these drugs avoided in the treatment and prevention of these
infections.
REFERENCES
1. Sobel J, Kaye D. Urinary tract infections. In: Mandell G, Bennett J, Dolin R, editors.
Mandell, Douglas, and Bennett’s: Principles and Practice of Infectious Disease. USA:
Elsevier; PA; 2010. p. 957–85.
2. Morgan MG, McKenzie H. Controversies in the laboratory diagnosis of community-acquired
urinary tract infection. Eur J Clin Microbiol Infect Dis., 1993; 12(7): 491-504.
3. Mody L, Juthani-Mehta M. Urinary tract infections in older women: a clinical review.
JAMA., 2014; 311(8): 844-54.
4. Nicolle LE, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM, et al. Infectious
Diseases Society of America guidelines for the diagnosis and treatment of asymptomatic
bacteriuria in adults. Clin Infect Dis., 2005; 40(5): 643-54.
5. Nicolle LE, Long-Term-Care-Committee S. Urinary tract infections in long-term-care
facilities. Infect Control Hosp Epidemiol., 2001; 22(3): 167-75.
6. Matthews SJ, Lancaster JW. Urinary tract infections in the elderly population. Am J Geriatr
Pharmacother., 2011; 9(5): 286-309.
7. Mazzulli T. Diagnosis and management of simple and complicated urinary tract infections
(UTIs). Can J Urol., 2012; 19 Suppl 1: 42-8.
8. Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect
Dis., 2001; 183 Suppl 1: S1-4.
9. Brown P, Ki M, Foxman B. Acute pyelonephritis among adults: cost of illness and
considerations for the economic evaluation of therapy. Pharmacoeconomics., 2005; 23(11):
1123-42.
10.Dielubanza EJ, Schaeffer AJ. Urinary tract infections in women. Med Clin North Am. 2011;
95(1): 27-41.
11.Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic
www.wjpr.net Vol 4, Issue 09, 2015.
308
12.Eriksson I, Gustafson Y, Fagerstrom L, Olofsson B. Prevalence and factors associated with
urinary tract infections (UTIs) in very old women. Arch Gerontol Geriatr., 2010; 50(2):
132-5.
13.Griebling TL. Urologic diseases in america project: trends in resource use for urinary tract
infections in men. J Urol., 2005; 173(4): 1288-94.
14.Bell LE, Mattoo TK. Update on childhood urinary tract infection and vesicoureteral reflux.
Semin Nephrol., 2009; 29(4): 349-59.
15.Das R, Perrelli E, Towle V, Van Ness PH, Juthani-Mehta M. Antimicrobial susceptibility of
bacteria isolated from urine samples obtained from nursing home residents. Infect Control
Hosp Epidemiol., 2009; 30(11): 1116-9.
16.Routh JC, Alt AL, Ashley RA, Kramer SA, Boyce TG. Increasing prevalence and associated
risk factors for methicillin resistant Staphylococcus aureus bacteriuria. J Urol., 2009; 181(4):
1694-8.
17.Gupta K, Hooton TM, Naber KG, Wullt B, Colgan R, Miller LG, et al. International clinical
practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in
women: A 2010 update by the Infectious Diseases Society of America and the European
Society for Microbiology and Infectious Diseases. Clin Infect Dis., 2011; 52(5): e103-20.
18.Drekonja DM, Johnson JR. Urinary tract infections. Prim Care., 2008; 35(2): 345-67, vii.
19.Hooton TM, Stamm WE. Diagnosis and treatment of uncomplicated urinary tract infection.
Infect Dis Clin North Am., 1997; 11(3): 551-81.
20.Kahlmeter G, Poulsen HO. Antimicrobial susceptibility of Escherichia coli from
community-acquired urinary tract infections in Europe: the ECO.SENS study revisited. Int J Antimicrob
Agents., 2012; 39(1): 45-51.
21.Warren JW, Abrutyn E, Hebel JR, Johnson JR, Schaeffer AJ, Stamm WE. Guidelines for
antimicrobial treatment of uncomplicated acute bacterial cystitis and acute pyelonephritis in
women. Infectious Diseases Society of America (IDSA). Clin Infect Dis., 1999; 29(4):
745-58.
22.Gupta K, Hooton TM, Roberts PL, Stamm WE. Short-course nitrofurantoin for the treatment
www.wjpr.net Vol 4, Issue 09, 2015.
309
23.Falagas ME, Vouloumanou EK, Togias AG, Karadima M, Kapaskelis AM, Rafailidis PI, et
al. Fosfomycin versus other antibiotics for the treatment of cystitis: a meta-analysis of
randomized controlled trials. J Antimicrob Chemother., 2010; 65(9): 1862-77.
24.Stamm WE, Counts GW, Wagner KF, Martin D, Gregory D, McKevitt M, et al.
Antimicrobial prophylaxis of recurrent urinary tract infections: a double-blind,
placebo-controlled trial. Ann Intern Med., 1980; 92(6): 770-5.
25.Nicolle LE. Prophylaxis: recurrent urinary tract infection in women. Infection., 1992; 20
Suppl 3: S203-5; discussion S6-10.
26.Mandell GL, Bennett JE, Dolin R. Mandell, Douglas, and Bennett's principles and practice
of infectious diseases. Churchill Livingstone/Elsevier; 2010.
27.Longo D, Fauci A, Kasper D, Hauser S, Jameson J, Loscalzo J. Harrison's Principles of
Internal Medicine, 18th Edition. McGraw-Hill Education; 2011.
28.Andreoli TE, Cecil RLF, Carpenter CCJ, Griggs RC, Loscalzo J. Cecil Essentials of
Medicine. 6th ed.: W.B. Saunders; 2004.
29.Ho PL, Yip KS, Chow KH, Lo JY, Que TL, Yuen KY. Antimicrobial resistance among
uropathogens that cause acute uncomplicated cystitis in women in Hong Kong: a prospective
multicenter study in 2006 to 2008. Diagn Microbiol Infect Dis., 2010; 66(1): 87-93.
30.Alos JI, Serrano MG, Gomez-Garces JL, Perianes J. Antibiotic resistance of Escherichia coli
from community-acquired urinary tract infections in relation to demographic and clinical
data. Clin Microbiol Infect., 2005; 11(3): 199-203.
31.Andrade SS, Sader HS, Jones RN, Pereira AS, Pignatari AC, Gales AC. Increased resistance
to first-line agents among bacterial pathogens isolated from urinary tract infections in Latin
America: time for local guidelines? Mem Inst Oswaldo Cruz., 2006; 101(7): 741-8.
32.Andreu A, Planells I, Grupo Cooperativo Espanol para el Estudio de la Sensibilidad
Antimicrobiana de los Patogenos U. [Etiology of community-acquired lower urinary
infections and antimicrobial resistance of Escherichia coli: a national surveillance study].
Med Clin (Barc)., 2008; 130(13): 481-6.
33.Shaban RA, Award AH, Abdullah MEE. Antibiotic Resistance pattern of urinary tract
isolates from outpatients in Sirte U Libia during the period 2005-2007. American J Infec
www.wjpr.net Vol 4, Issue 09, 2015.
310
34.Ladhani S, Gransden W. Increasing antibiotic resistance among urinary tract isolates. Arch
Dis Child., 2003; 88(5): 444-5.
35.Louie L, Majury A, Goodfellow J, Louie M, Simor AE. Evaluation of a latex agglutination
test (MRSA-Screen) for detection of oxacillin resistance in coagulase-negative