Effect of a structured teaching program in the
evaluation of and perception of Inguinal Hernia by
Phase III M.B.B.S. students – A cross sectional study
Riju Ramachandran, Vimaladhithan Mahendran, Naveen Sivadas
Department of General Surgery, Amrita Institute of Medical Sciences, Amrita Viswavidyapeetham, Kochi, Kerala
Abstract
Background: It is a myth that the student knows the anatomy, causes, sequelae, complications and types of hernia. Though educational tools for the surgical procedure are available but a structured teaching format is not described in literature. A structured methodology of teaching may help in improving the knowledge of the student.
Methods: A cross sectional study was done at our institution using 37 Phase III MBBS students. A pre-test was followed by a structured methodology of teaching students about inguinal hernia. A post-test and feedback was taken after 2 days. Data was computed. Statistical significance was found by using non-parametric test – Wilcoxon Signed-Ranks test. The quantitative data were expressed as Mean ± SD and qualitative data were expressed as frequency and proportions.
Results: Mean marks of the students were 4.37 and 5.11 among 8th and 9th semester students which improved to
15.04 and 14.33 marks which was statistically very highly significant with p = 0.0001 and 0.008 respectively which showed a gain in knowledge of students.
Conclusion: Structured teaching improves the ability of an IMG to diagnose hernia. Objective Structured Teaching Evaluation (OSTE) will help the teacher, whether junior or senior, learn to be a better teacher.
Key words: Hernia, Medical Education, Structured teaching, under graduate medical students
Address for Correspondence: Dr. Riju Ramachandran
AG1, Sterling Sarovar Apartments, Kosseri Lane, Edapally, Kochi, Kerala E-mail: [email protected]
Introduction
Inguinal hernia is very common in the community and in the surgical OPD. It is a common procedure done by the surgeon and accounts for 15% - 18% of all surgical procedures[1]. Given the complexity of its
surgical anatomy and understanding, our experience is that teaching of this subject is often inadequate. Right from the anatomy of the inguinal canal to the descriptions of the different types of hernia: inguinal, direct / indirect, femoral hernia, and rare hernias, there is confusion among students. The sad fact is that most students fare poorly in their exams due to their poor understanding of the subject. It is essential for the MBBS student to have knowledge of the clinical features leading to diagnosis of the problem. The students are introduced to the anatomy of the groin in their first and second semesters. During the third semester rotation in surgery they are exposed to the
clinical examination including the history taking and physical examination. A large part of the knowledge the students attain is by seeing and examining patients during out-patient (OP) clinics or bedside teaching. Often they are given a lecture class on groin hernia during the third, fifth or seventh semesters. This system is prevalent in India and even in most western countries.
A large subset of Indian Medical Graduates (IMG) are incompetent in their understanding of inguinal hernia. Many of these cases are missed by practitioners and present later with complications. A structured teaching format is not available in literature[2,3]. There
its complications. In practical exams the student often gives a diagnosis of hernia as “Inguinal hernia” when it should be given in a more complete format as “Unilateral / bilateral, inguinal / femoral, complete / incomplete, direct / indirect, reducible / irreducible, complicated / uncomplicated, enterocele / bubunocele / omentocele with / without Chronic Obstructive Pulmonary Disease (COPD) / Benign Prostatic Hypertrophy (BPH) / Rectal lesion”[4]. Often causative factors like weight lifting,
COPD, BPH or rectal lesions are left undiagnosed and patient after hernia surgery presents with late stage disease like Carcinoma rectum, Ca Prostate which could have been diagnosed and managed early. An indicator of the students’ ability to understand anatomy of groin hernia is in the ability to differentiate & discuss the difference between direct and indirect inguinal hernia. This ability is useful to plan surgical approach and navigation during repair. The direct and indirect inguinal herniae have different pathogenesis. The indirect hernia does not require a mesh insertion in all cases, but the direct hernia definitely does. Our main objectives were to assess whether a structured teaching will improve the ability of the student to diagnose hernia and to understand the student perception towards the structured learning.
Materials and Methods
A cross sectional study was done on phase 3 MBBS students (8th and 9th Semester) at our institution
presently doing rotation in the department of General Surgery. Final year MBBS students who have already completed one posting in General Surgery were included. Students who did not give consent to participate in the program and students who were absent on the day of the pretest or post-test were excluded. Inclusion criteria was on the assumption that final year students have already completed one posting in General Surgery in their third semester at which time all aspects of evaluation of hernia have already been covered by regular method of teaching . Sample size: A similar study conducted for effectiveness of teaching the topic of hernia could not be found on literature review. A sample size determination was hence difficult for this study. We conducted a pilot study using 8 random students from one batch posted in the department , testing for level of knowledge by giving a set of questions on the topic. The marks obtained by these students were very low with an average score of 4 out of 16. The maximum score obtained was 6 and minimum of 3 marks. A post test conducted after structured teaching for these students
17).Since the variablity of marks was less and all the students got low scores in pretest and grossly increased marks in post test, it was determined that small sample size of 16 itself could give high precision with a confidence level of about 95%. To improve on the level of confidence we planned to conduct this study with 16 students each from 8th and 9thsemester
MBBS students posted in surgery department (n=32). However while conducting the study we had 46 students from 8th semester and 9 students from 9th
semester participating, thereby increasing the number of students to 55. 18 students were excluded due to absence or lack of consent giving a sample size of 37.
Methodology Used: Clearance was obtained from the Institutional review board prior to starting the project. Informed consent was taken from all the students enrolled in the study. All the students included in the study were initially subjected to a pretest consisting of Multiple Choice Question’s (MCQ) and a Short answer question (SAQ). The questions were structured in such a way as to cover anatomy of abdominal wall and inguinal canal, clinical features, complication, types of and treatment of inguinal hernia. There was a single SAQ on complete diagnosis. The total marks out of a maximum of 21 marks obtained were tabulated in Microsoft excel.
Names and other personal details were avoided in the answer sheets. Students were asked to write down only their roll number so as to compare the pre-test and post-test results. The students were first given a small session as preview of how a structured class on the topic will be taken. The students were then subjected to a focused, structured session on all aspects of groin hernia.
We provided three components of structured teaching methodology by engaging a small group of students over 2-3 hours in a large well lit, quiet, lecture hall with an interactive session using various teaching modalities and tools increasing the receptiveness of the students[8].
1. Physical structure: They were taken to a quiet, well-lit classroom area. The class was for 3 hours equally divided among the various aspects of the condition. This included various aspects of anatomy of the abdominal wall and the inguinal canal, clinical features of inguinal hernia including clinical demonstration of signs, types of hernia, complications, sequelae and Surgery for inguinal hernia.
PowerPoints, posters, photographs of anatomical structures, videos of operative procedures, whiteboard and writing board, the condition was discussed. The students were told of the schedule of the program at the start of the session keeping them aware of what would happen next.
3. Teaching component: An Assistant professor and three surgical residents discussed the condition with the students, the author intervening and facilitating discussion and learning at regular intervals during the session. Students were asked to interact with the teachers and with each other during the class regarding their concept of, understanding of and doubts on the topic. The pre-test question paper was also discussed at relevant areas of the interaction.
Two such sessions were taken separately on separate days-Initially for the eighth and then the ninth semester students. A post test was conducted after 2 days of session giving the same set of questions as the pretest. The students were given a separate feedback form. Components assessed were the content of the session, structure of the program, quality of the teacher, quality of the presentation and overall satisfaction with the session. Take-home points as understood by the student and suggestion for improvement was obtained as open ended feedback. No identifying information was taken on the feedback form.
Data Management and Statistical Analysis: The collected data were compiled by using Microsoft Excel 2010 and were analyzed by using statistical software SPSS 20.0 version.
Statistical Analysis: The qualitative data were expressed as frequency and proportions and quantitative data were expressed as mean ± SD. The
statistical significance between pre-test and post-test for effectiveness of structured teaching in diagnosis of inguinal hernia among final year (8th and 9th Semester)
undergraduate medical students was found by using non-parametric test – Wilcoxon Signed Ranks test since the sample size in each of the groups was less than 30. Level of Significance: P – value < 0.05 was considered as statistically significant.
Results
In our present study we have totally included 46 under graduate medical students ie., from 8th Semester
(n)=28 and in 9th semester 9 students, and excluded 18
students for various reasons. Hence, we have included totally 37 students for this study. Comparison between pre-test and post-test for effectiveness of structured teaching in diagnosis of inguinal hernia among final year (8th Semester and 9th semester) undergraduate
medical students are shown in Table 1and Figure 1.
Figure 1. Distribution of students’ scores in pre and post test results
Eight Semester Ninth Semester
0 2 4 6 8 10 12 14 16
Pre test Post test
Table 1. Distribution of students, mean and SD of marks in pre and post test results
Test No. of Students (N) Mean Marks Std. Deviation Z - Value P – value & Significance
Pre-test
8th Semester 27 4.37 1.497
-4.553 0.0001
< 0.001 Post-test
8th Semester 28 15.04 1.895
Pre-test
9th Semester 9 5.11 2.619
-2.670 0.008
< 0.01 Post-test
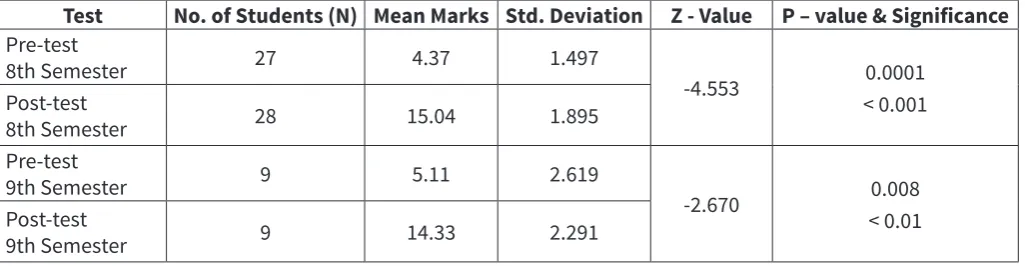
The knowledge scores of under graduate medical students were 8th semester: pre-test 4.37 ± 1.50 and in
post-test 15.04 ± 1.90 and 9th semester: pre-test 5.11 ±
2.62 and in post-test 14.33 ± 2.29. The Wilcoxon Signed Rank Test Z – value = -4.553 with P – value < 0.001 and Z – value = -2.670 with P – value < 0.01 respectively for 8th and 9th semester students were statistically highly
significant. This result shows that structured teaching in diagnosis of inguinal hernia among final year (8th semester) undergraduate medical students has been effective and knowledge of the students on the topic drastically increased.
Analysis of Feedback Form
A feedback form (Annexure) based on Likert scale was filled up by the students after the post test. The parameters assessed were content of the program, structure of the program, quality of presentation and presenter. Two more aspects were take home message and suggestion for improvement.
Content - parameters assessed were: a. if content was interesting
b. if content was understandable
c. was there clarity in the presentation content d. did the student gain knowledge.
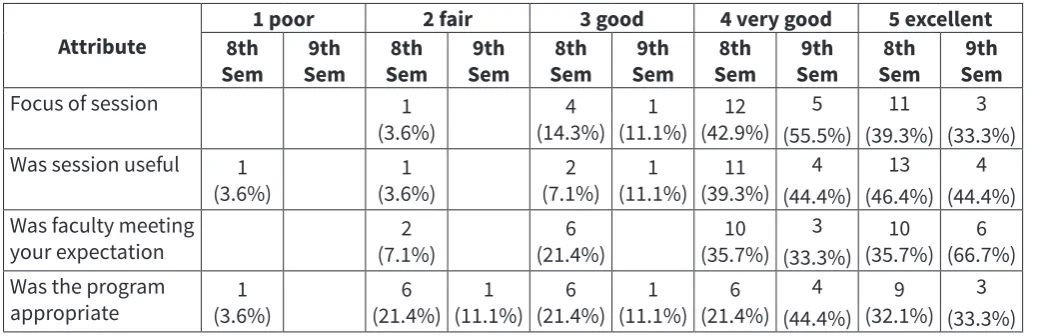
All the eighth and ninth semester students answered in the affirmative for all the four queries (Table 2). Structure: This part of the feedback was on parameters like Focus of lecture, usefulness of lecture, did lecturer meet expectations and was the presentation appropriate (Table 3).
Feedback for the methodology and performance of the teacher is depicted in table 4.
All the ninth semester students were satisfied with the lecture and felt that the program answered their questions. Except for three students all other eighth semester students were satisfied and felt that this session helped them understand the topic better. Overall impression of the program was also very good or excellent for most students in both 8th and 9th
semesters. More than 60% of the students from both the semesters perceived that the take home message understood anatomy, diagnosis and types of hernia. Most students were confident about management options of inguinal hernia after the session.
Table 2. Feedback from the students about the content
Attribute number Total
8th sem
Actual
number percentage
Total number 9th sem
Actual
number percentage
Attended class 38 28 73.7 9 9 100%
Liked content of program 28 28 100% 9 9 100%
Felt content was understandable 28 28 100% 9 9 100%
Felt there was clarity 28 28 100% 9 9 100%
Gained knowledge 28 28 100% 9 9 100%
Table 3. Feedback from the students on the program
Attribute 8th 1 poor 2 fair 3 good 4 very good 5 excellent
Sem Sem9th Sem8th Sem9th Sem8th Sem9th Sem8th Sem9th Sem8th Sem9th
Focus of session 1
(3.6%) (14.3%)4 (11.1%)1 (42.9%)12 5 (55.5%)
11 (39.3%)
3 (33.3%) Was session useful 1
(3.6%) (3.6%)1 (7.1%)2 (11.1%)1 (39.3%)11 4 (44.4%)
13 (46.4%)
4 (44.4%) Was faculty meeting
your expectation (7.1%)2 (21.4%)6 (35.7%)10
3 (33.3%)
10
(35.7%) (66.7%)6 Was the program
appropriate (3.6%)1 (21.4%)6 (11.1%)1 (21.4%)6 (11.1%)1 (21.4%)6 4 (44.4%)
9 (32.1%)
Suggestions from students and take home message:
These were two other parameters in the feedback form. On analysing this we found that in more than 80% of the students in the eighth semester perceived take home message was understood anatomy and diagnosis. None of the 9th semester students gave
anatomy as their take home message rather they felt the take home message was types of hernia, diagnosis of hernia and surgical options possibly because they may be exam going students. Around 60 % of the students felt that they understood the different types of hernia.
Suggestion for improvement the students gave were
• To increase the number of such events and for other topics also.
• More use of videos especially for surgical procedures.
• Few students did not like the PowerPoint and have suggested avoiding PowerPoint slides in such a program. They also wanted the teacher to be more interactive and use the writing board more.
• More time to be given for such a session. Students felt that the 2-3 hours spent was a very short time.
• Many students wanted us to include a test after each topic and subtopic.
• Few students felt that instead of interacting they should be given time to write notes indicating a resistance to change their methodology of learning.
Discussion
Education involves the building of concepts. These concepts are received through various modes of teaching. A student must be able to classify, organise, relate and distinguish between experiences to form ideas[5] Apart from having a solid intellect the
surgeon should have skill, ability, behavior and the right attitudes[6]. Surgeons are said
to be operating physicians. Due to the complexity of
the anatomical structure, the anatomy of the inguinal canal is very difficult to understand and explain to medical students and surgical residents[7]. Though
an appropriate clinical diagnostic algorithm for the accurate diagnosis of groin hernia is depicted in every textbook on Surgery, many students fail to attain competence in diagnosing the condition. There is often a very shallow understanding of many aspects of hernia causing this failure.
A review of literature showed the definition of structured teaching as “Structured teaching addresses challenging behaviors in a proactive manner by creating appropriate and meaningful environments that reduce the stress, anxiety and frustration which may be experienced by students”[8]. There are many problems
causing difficulty in learning for the students like a difficulty understanding a language, distractions, organizational difficulty, and a general resistance to change. As suggested by the requirement of structured teaching in a paper on autism by Susan Stokes[8] all the
three components namely Physical structure, Visual schedule and teaching components were addressed in our project. We modified the requirements to suit the learning of our MBBS students for the program on inguinal hernia.
In our study we find that students who are in eighth and ninth semester MBBS have attained very poor scores when a test on the topic of hernia was given. When the test was taken after the structured teaching on the topic the mean marks improved significantly. This result being statistically significant ratifies our research question. There are no such results available in the literature on a similar topic. But one study by Carlos et al[6] have shown significant improvement
among 46 instructors who were trained to teach surgical residents to perform Hernioplasty in Brazil. A focussed session on the topic explaining the various aspects of the problem at hand definitely improves the level of knowledge of the learner. Facilitating learning by discussing the mistakes made in the
Table 4. Feedback from the students on faculty
Feedback on faculty
1 poor 2 fair 3 good 4 very good 5 excellent
Semesters
8th 9th 8th 9th 8th 9th 8th 9th 8th 9th
question paper also may have helped in improving the knowledge levels. We had one SAQ to give the diagnosis of the hernia with a weightage of 6 marks. All students failed in the pretest with only a few writing a diagnosis as “Inguinal hernia”. But post session SAQ showed the answer written correctly including all the six components in more than 80 % of the students, Few students could still give 4 -5 components only after the session.
Content of the program was liked by all the students both eighth and ninth semester. For the structure of the program, most of the eighth semester students (81%) felt that the program was well focussed on the topic and 85% of the students felt it was useful to them. 45% of the students in eight semester felt that the program was not appropriate. These were the students who felt the need for more videos, and less use of PowerPoint slides. Ninth semester students were more positive as compared with the eighth semester in the feedback on the faculty. We even got a few negative remarks from the eighth semester students. Few students felt that this session was no better than the regular class. When the program was being conducted for the eighth semester students there was more of interaction by the junior faculty. Senior faculty interaction in teaching was lower for these students. The students wanted more interactive sessions. Some students did not like the mode of presentation.
For the ninth semester students, we increased the involvement of senior faculty including the author and found a significantly better faculty feedback. Since the numbers are small, we will not be able to comment on the relevance of this feedback. Most students felt that teaching surgical subjects needed more videos on the surgery along with the pictorial representation. We provided this by engaging a small group of students over 2-3 hours in a large lecture hall with an interactive session using various teaching modalities and tools increasing the receptiveness of the students.
Video presentations and powerpoint slides enhance students’ understanding of and interest in surgical procedures[9]. The blackboard and the interactive
whiteboard are increasingly being used in teaching surgical procedures to the students. 3D displays, LCD can also be used as adjuncts with the writing board for interactive teaching and learning[10]. There
is no doubt that these tools help to maintain interest in the students and increase the receptivity of the students to very complex ideas and surgeries[7]. The
feedback from the students also reiterates this fact.
process may increase the levels of knowledge of the students[11]. This is an option we can try in future
projects on teaching learning. Surgery is presently learnt on an apprenticeship model over few years as and when a real patient is seen by the student on day to day basis[11]. The learning experience may be
inadequate due to the fear of complication or failure. Human anatomy and surgery are difficult to teach due to complexity of procedures, risk of complications, non-availability of dead bodies, legal and ethical issues. Simulators are now being used extensively in many medical colleges for teaching anatomy[12].
Structured teaching of a condition integrating various aspects of the problem utilising multiple tools can help in increasing the knowledge levels of the student. It can be rewarding to the teachers also.
We feel the validity of our results has increased due to the higher number of students inducted in the study. Feedback on the faculty attained from such sessions can help us improve our methodology of teaching. It can be a rewarding and very satisfying experience overall to the teachers. Some authors have recommended an Objective Structured Teaching Evaluation (OSTE) for assessing the teaching ability of the faculty[13].In our study there was an overall
satisfaction of the performance of the faculty. There was not a single negative remark on the faculty by the senior ninth semester students. Majority of the students opined that the faculty performance was very good or excellent (>90%). Few of the Eighth semester students felt that the faculty was less enthusiastic, the session was no different from a regular lecture and that the faculty interaction with the students was inadequate. In this group of students the sessions were taken more by the residents and the author was facilitating the learning process. The residents may have been lacking in experience as to conduct of a teaching learning session. An OSTE on these junior residents with a feedback given to them will improve their ability to teach. It will show them the flaws in their methodology and give them inputs to improve. Regular sessions with OSTE for the faculty and residents will help improve their teaching skills. Mathew Zackoff et al have opined that use of an objective, observable, measurable and reproducible OSTE improves the resident’s skill in teaching and helping them become better doctors[14]. In teacher training courses OSTE may
their postgraduate residency they may be subjected to session of OSTE with standardised students and environments so that they can be assessed for their teaching skills[15]. Feedback is immediate and it
gives inputs to the residents as to areas they need to improve, to enhance their skill of teaching.
Conclusion: Hernia is a very common condition in surgical practice needing good clinical skills in diagnosis and management. A structured teaching using multiple tools and integrated teaching of various aspects of the problem will improve the ability of an IMG to diagnose the condition. There is a statistically significant increase in the level of knowledge of the students after the structured teaching which shows that this modality of teaching is effective in teaching students the various aspects of hernia. It could be extended to other regions and conditions as well. Students understood the anatomy of the hernia better. Though all the students failed to give a correct diagnosis in the pre-test, students were able to give a correct, complete diagnosis of hernia after the session. A proper understanding of the types of the hernia was obtained. The students were very positive about the session in helping them learn and effectively diagnose inguinal hernia. Most students want more such sessions using more audiovisual aids. Students had a lesser liking for power point slides and preferred white or black board writing. They were also more in favour of videos as teaching material for operative surgery. Simulation may add another dimension to this teaching modality.
The students had a more negative feedback with junior faculty and a more positive feedback when senior faculty facilitated the learning process. OSTE will help the teacher, whether junior or senior, learn to be a better teacher giving inputs to areas requiring improvement.
References
1. Sangwan M, Sangwan V, Garg M, Praveen M, Garg U. Abdominal wall hernia in a rural population in India-Is spectrum changing? O J Epi 2013,3:135-138. Available on: http://dx.doi.org/10.4236/ ojepi.2013.33020. DOI: 10.4236/ojepi.2013.33020
2. Khatib M, Hald N, Brenton H, Barakat MF, Sarker SK et al. Validation of open inguinal hernia repair simulation model: a randomized controlled educational trial. Am J Surg 2014;208(2):295–30 PMID: 24581993 3. Mann BD, Seidman A, Haley T, Sachdeva AK. Teaching three-dimensional
surgical concepts of inguinal hernia in a time-effective manner using a two-dimensional paper-cut. Am J Surg 1997;173(6):542-5.
4. Amerson JR. Inguinal Canal and Hernia Examination. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 96. Available on: https://www.ncbi.nlm.nih.gov/books/NBK423. PMID: 21250263
5. Dale Edgar. Audiovisual methods in teaching. Ny: Dryden Press, 1946.
6. Carlos José lazzarini; Adhemar Monteiro Pacheco Júnior,Bárbara Bozzoli destro; Caroline Tamaro; Fábio Antonio del Picchia et al. Systematic training model for teaching, development and training of instructors in inguinal hernia treatment using the Lichtenstein technique. Hernia campaign 2014 & 2015. Rev. Col. Bras. Cir 2016;43(5):382-91. DOI:10.1590/0100-69912016005018
7. Skandalakis JE, Colborn GL, Androulakis JA et al. Embryologic and anatomic basis of inguinal herniorrhaphy. Surg Clin North Am 1993;73(4):799-836. PMID: 8378822
8. Susan Stokes. Structured Teaching: Strategies for Supporting Students with Autism? “Written by Susan Stokes under a contract with CESA 7 and funded by a discretionary grant from the Wisconsin Department of Public Instruction”. Available on: https://www.cesa7.org/sped/autism/ structure/str10.htm
9. Hotokezaka M, Chijiiwa K, Kondo K, Kai M et al. Video monitoring and slide and video presentations as tools for surgical education. Hepatogastroenterology 2008;55(86-87):1519-22.
10. Fry H, Kneebone R. Current and future simulation and learning technologies. In: Surgical Education: Theorising an Emerging Domain. Springer Science & Business Media 2011;8:25. ISBN: 978-94-007-1682-7 11. Luca Ansaloni, Fausto Catena, Federico Coccolini, Marco Ceresoli,
Antonio Daniele Pinna. A Low-Cost Teaching Model of Inguinal Canal: A Useful Method to Teach Surgical Concepts in Hernia Repair. Univ J Edu Res 2014;2(4):375-378 Available on: http://www.hrpub.org DOI:10.13189/ ujer.2014.020405
12. Dent JA. Current trends and future implications in the developing role of clinical skills centers. Med teach 2001;23(5):483-9 PMID: 12098370 13. Trowbridge RL, Snydman LK, Skolfield J et al. A systematic review of the
use and effectiveness of the Objective Structured Teaching Encounter. Med Teach 2011;33(11):893-903. DOI: 10.3109/0142159X.2011.577463 14. Zackoff M, Jerardi K, Unaka N, Sucharew H, Klein M. An Observed
Structured Teaching Evaluation Demonstrates the Impact of a Resident-as-Teacher Curriculum on Teaching Competency. Hospital Pediatrics 2015;5(6): 342-347. DOI: 10.1542/ hpeds.2014-0134
15. Katherine Julian, Nicole Appelle, Patricia O’Sullivan, Elizabeth H. Morrison & Maria Wamsley. The Impact of an Objective Structured Teaching Evaluation on Faculty Teaching Skills. Teaching and Learning in Medicine 2012;24(1):3-7. Available on: https://www.tandfonline.com/ doi/abs/10.1080/10401334.2012.641476
Date received: October 31st 2018 Date accepted: December 28th 2018