LEABHARLANN CHOLAISTE NA TRIONOIDE, BAILE ATHA CLIATH TRINITY COLLEGE LIBRARY DUBLIN
OUscoil Atha Cliath
The University of Dublin
Terms and Conditions of Use of Digitised Theses from Trinity College Library Dublin
Copyright statement
All material supplied by Trinity College Library is protected by copyright (under the Copyright and
Related Rights Act, 2000 as amended) and other relevant Intellectual Property Rights. By accessing
and using a Digitised Thesis from Trinity College Library you acknowledge that all Intellectual Property
Rights in any Works supplied are the sole and exclusive property of the copyright and/or other I PR
holder. Specific copyright holders may not be explicitly identified. Use of materials from other sources
within a thesis should not be construed as a claim over them.
A non-exclusive, non-transferable licence is hereby granted to those using or reproducing, in whole or in
part, the material for valid purposes, providing the copyright owners are acknowledged using the normal
conventions. Where specific permission to use material is required, this is identified and such
permission must be sought from the copyright holder or agency cited.
Liability statement
By using a Digitised Thesis, I accept that Trinity College Dublin bears no legal responsibility for the
accuracy, legality or comprehensiveness of materials contained within the thesis, and that Trinity
College Dublin accepts no liability for indirect, consequential, or incidental, damages or losses arising
from use of the thesis for whatever reason. Information located in a thesis may be subject to specific
use constraints, details of which may not be explicitly described. It is the responsibility of potential and
actual users to be aware of such constraints and to abide by them. By making use of material from a
digitised thesis, you accept these copyright and disclaimer provisions. Where it is brought to the
attention of Trinity College Library that there may be a breach of copyright or other restraint, it is the
policy to withdraw or take down access to a thesis while the issue is being resolved.
Access Agreement
By using a Digitised Thesis from Trinity College Library you are bound by the following Terms &
Conditions. Please read them carefully.
RETROSPECTIVE ANALYSIS OF DENTAL IMPLANTS PLACED OVER
A 6 YEAR PERIOD, COMPARING OVERDENTURES AND IMPLANT
FIXED COMPLETE DENTURES, IN TERMS OF PATIENT
SATISFACTION AND QUALITY OF LIFE .
MAIRE BRENNAN
D. Ch. Dent.
DIVISION OF RESTORATIVE DENTISTRY AND PERIODONTOLOGY,
SCHOOL OF DENTAL SCIENCE,
TRINITY COLLEGE,
j^ T R lN iT Y C O L L E G E ^
0 8 j.AN 2 n r
Declaration
This thesis has not been subm itted as an exercise fo r a degree at any o th er university.
Except w h ere stated, th e w ork described th erein was carried out by me alone.
Page
Acknowledgements
iii
Summary
iv
Contents
viii
Index of figures
xi
N - * ■ r - i» -■
.A
«W ' ':
A
f'l ■ ^
■ ■
Aknowledgements
M y s u p e rv is o r P ro fe s s o r O 'C o n n e ll h e lp e d to c o n c e iv e th is s tu d y an d a d v is e d an d m o tiv a te d
t h e p ro d u c tio n o f all t h e w o r k in v o lv e d in it. F or th is an d m u c h m o re , I o w e h im a h u g e d e b t o f
g r a titu d e .
All T u to rs o f t h e p ro s th o d o n tic p r o g r a m m e , w h o h a v e im p ro v e d m y a b ility a n d c o n fid e n c e
b e y o n d re c o g n itio n , M ic h a e l O ' S u lliva n , F ran k H o u s to n , G e rr y C le a ry , C o lm S u g ru e , A n n e
G u n d e rm a n a n d F ran k Q u in n . T h a n k y o u all f o r th e t im e an d e f f o r t s p e n t passing o n y o u r
k n o w le d g e a n d e x p e rie n c e .
D r. A lan K elly a n d P ro fe s s o r N o e l C la ffe y , fo r t h e ir h e lp w ith t h e s ta tis tic a l an alysis.
T h e s ta ff o f m e d ic a l re c o rd s f o r t h e ir h e lp w ith d a ta c o lle c tio n .
All P o s tg ra d u a te s tu d e n ts , e s p e c ia lly w ith in t h e p ro s th o d o n tic p ro g r a m m e , as s h a rin g w a s
m o re e n jo y a b le .
M y fa m ily to w h o m I a m tr u ly g r a te fu l.
F in ally, I w o u ld like to d e d ic a te th is th e s is to m y fia n c e Jc, f o r his c o n s ta n t lo v e , s u p p o rt an d
Summary
study Objectives:
The aim of the first part o f this project was to construct an implant
database that recorded the details of every implant placed and restored in the Dublin Dental
Hospital over a 6 year period. The objective o f the second part of the study was to assess and
compare patient satisfaction and oral health related quality of life (OHRQOL) in patients
treated with complete implant fixed prostheses and removable implant prostheses
(overdentures) in the Dublin Dental Hospital during this time frame. The specific aims were to
report on patient satisfaction in terms of (1) patient perceptions o f selected technical aspects
o f treatm ent outcome, (chewing function, comfort, speech, cleansability ) (2) patient
perceptions o f treatm ent experience, (3) incidence of complications, and (4) certain patient
demographic factors such as patient sex.
Materials and Methods:
Surgical day-lists were hand-searched to compile a list of patients
who had dental implants placed between January 2000 and January 2006. This was then cross
referenced w ith an electronic search o f 'Salud', the hospital's electronic patient record system,
using the term 'dental implant' as the search criterion. The charts for these patients were then
hand searched and the following information was entered into a spread sheet; name, age,
implant type, length, diameter, site and prosthesis type.
This database served to identify our study population for the second part of the study, namely,
a complete implant fixed prosthesis group (mean age 56,12 males, 25 females) and an implant
overdenture group (mean age 57.5,11 males, 14 females). A 27-item, self-administered,
structured multiple response questionnaire including the Oral Health Impact Profile-14
measurement tool and a patient satisfaction survey was used as the instrument for this study.
Results: 1111 im plants were placed in 452 patients during the period January 2000 to January
2006. The 1111 im plants supported 731 prostheses, 74% o f which were single im plant
restorations, 7% fixed partial dentures, 12% Im plant overdentures and 7% im plant fixed
com plete denture prostheses. The mean age o f the patients w ho received dental im plants was
53.4 years. The m ost com m on age group th a t received dental im plants was th e 40 to 60 year
olds, w ith 38.5% o f the to ta l num ber o f im plants being placed in this group.
Generally, p a tient satisfaction was very high in both the im plant overdenture and fixed
com plete denture groups. In the 'overall satisfaction' category, the median scores fo r th e fixed
and rem ovable groups were 1 (to ta lly satisfied) and 2 (very satisfied) respectively. In f a c t , the
m a jo rity o f categories in the p a tient satisfaction questionnaire had median scores o f 1 (to ta lly
satisfied) or 2 (very satisfied) and no category had a median score o f 4 (unsatisfied) o r 5 (Not
at all s a tis fie d ). The high overall satisfaction median scores are sim ilar to anothe r study
carried o u t by Allen and M cM illan who reported a median o f 2 (very satisfied) in the general
satisfaction dom ain fo r patients who received a fu ll arch im plant prosthesis (fixed or
rem ovable) [84].
W hile subjects in the removable im plant overdenture group reported low er overall
satisfaction than the fixed com plete denture im plant group fo r the m ajo rity o f categories
(aesthetics, chewing capacity, speech, discom fort w ith surgical/restorative procedures,
com plications, and length o f tim e tre a tm e n t took), statistical analysis (W ilcoxon rank sums
test) revealed a significant difference between the tw o groups only w ith regards to overall
satisfaction, chewing capacity and aesthetics, w ith the im plant overdenture group being less
satisfied w ith these parameters. In just three categories; cost, satisfaction w ith tre a tin g doctor
and a b ility to perform oral hygiene measures, the fixed group were less satisfied than the
rem ovable group, but the difference was not found to be statistically significant (W ilcoxon
In g e n e ra l, p a tie n ts w ith a fixed prosthesis had a very good OHRQOL . The m ed ian score fo r
th e fixed g ro up w as 2 (indicating p a tie n ts 'h a rd ly e v e r' exp erien ced problenns) in all th e OHIP
dom ain s, w ith th e exception o f 'physical pain' which had a m ed ian score o f 3 (indicating
p a tie n ts 'occasionally' exp erien ced p roblem s ). The m ed ian score fo r th e re m o v a b le g ro up was
4 (ind icatin g th a t p a tie n ts e xp erien ced p roblem s 'v e ry o fte n ') in all dom ains a p a rt fro m 'social
d isability' and 'h a n d ic a p '. In th e s e dom ains, th e m ed ian score was 2 ( indicating p atien ts
'h a rd ly e v e r' e x p erien ced p ro b lem s).D esp ite th ese re s u lts , a statistically significant d iffe re n c e
b e tw e e n th e tw o groups was only fo u nd in th e psychological d isco m fo rt and psychological
disab ility dom ain s (W ilcoxon rank sums t e s t ) indicating th a t o verall th e d iffe re n c e in OHRQOL
b e tw e e n th e groups m ay not be very large.
Regardless o f a m ed ian score o f 'very satisfied ' being re p o rte d w ith regard to com plications
e x p e rie n c e d in both th e fixed and re m o v a b le groups, th e n u m b e r o f com plications actually
e x p e rie n c e d was q u ite high in th e re m o v a b le group. A higher p erc e n ta g e (52% ) o f th e p atien ts
w h o received an o v e rd e n tu re prosthesis exp erien ced a t least o ne com p licatio n co m p ared to
th e fixed c o m p le te d e n tu re prosthesis group (32% ). The average fo llo w up periods w e re 2 5 .5
m o n th s (range o f 3 to 6 6 m onths) and 2 4 m onths (range 3 -8 0 m o n th s) fo r th e o v e rd e n tu re
and fixed groups respectively. T he m ost co m m o n com plications w e re soft tissue re la te d (
o v e rd e n tu re 4 4 % , fixed 13.5% ) and m echanical com plications (o v e rd e n tu re 36% , fixed 8% ).
C onclusions: G en erally, p a tie n t satisfaction w as high in both th e im p la n t o v e rd e n tu re and
fixed c o m p le te d e n tu re groups. Patients w ith re m o v a b le im p la n t o v e rd e n tu re prostheses had
statistically significant lo w e r overall satisfaction, as w ell as lo w e r satisfaction w ith th e chew ing
capacity and aesthetics o f th e ir prostheses co m p ared to patien ts w ith c o m p le te fixed im p la n t
prostheses.
In g e n e ra l, p a tie n ts w ith a fixed prosthesis had b e tte r OHRQOL th a n p atien ts w ith re m o v a b le
psychological d isco m fo rt and psychological disability dom ains o f th e oral health im p a c t pro file
(O H IP -1 4 ) q uestio n naire.
Patients w ith re m o v a b le im p la n t o v e rd e n tu re s experienced m o re com plications th a n patien ts
w h o received c o m p le te fixed im p la n t prostheses, o v e r a sim ilar tim e period.
Due to th e respective n a tu re o f this study, p a tie n t allocation to th e tw o groups was not
ra n d o m ize d . T h e re fo re , it w o u ld be in a p p ro p ria te to in fer th a t th e d ifferences b e tw e e n th e
groups could only be ascribed to th e tr e a tm e n t in te rv e n tio n . To o verco m e th e d ifficulties
associated w ith ethical approval fo r ra n d o m iza tio n , a p rospective w ith in subject cross-over
tria l w h e re each p a tie n t receives both ty p e o f prostheses fo r a period o f tim e w o u ld be helpful
Table of Contents
C hapter 1: In tro d uctio n ...1
O bjectives...2
C hapter 2: Literature R eview ...4
O utcom e M easures... 4
Im p lan t Survival/Success... 4
Survival/Success Criteria... 5
Patien t Centred Outcomes... 6
P atien t Satisfaction...8
Oral H ealth Related Q uality o f Life... 8
Studies Relating to Oral H ealth Related Quality o f Life...10
Oral H ealth Im pact P r o file ... 13
Fixed Prostheses... 14
R em ovable Prostheses... 18
Choice o f Prosthesis... 22
Prosthesis Survival/Success...23
O perator Education...26
Cost... 27
Patient Preference... 27
Im p la n t Com plications... 28
Fixed Prostheses... 28
Chapter 3: Materials and M e th o d s ... 35
Study Design... 35
Im plant Database...36
Sampling Procedure... 37
Study Population... 37
Ethical Considerations... 38
Data Collection... 39
OHIP...40
Patient Satisfaction Questionnaire... 41
Dental Record Data Abstraction... 43
Statistical Analysis... 44
Chapter 4: Results...46
Im plant Database... 46
Patient Satisfaction Questionnaire... 50
Patient satisfaction (maxilla only)... 56
OHIP Questionnaire... 63
OHIP Questionnaire (maxilla only)... 67
Complications (Implant Overdentures)...69
Complications (Implant Fixed Complete Dentures)...70
Chapters: Discussion...72
Database Results... 72
No o f im plants placed...72
Prostheses types... 73
A natom ical D istribution o f im p la n ts...74
Patient Satisfaction Survey...74
Patient Satisfaction (maxillary sub-group)... 77
OHIP as measurement tool...78
Oral health Related Quality of Life... 78
Complications...81
Study Limitations... 83
Conclusions... 85
References... 86
List of Figures
Figure 1: Im p la n t Success C riteria proposed by A lbrektson 1 9 86.
Figure 2: Locker's m o d el o f oral h ealth (Locker 1 9 8 8 ).
Figure 3: M a x illa ry and m a n d ib u la r fixed c o m p le te im p la n t prostheses.
Figure 4: Fitting surface o f m a n d ib u la r fixed prosthesis.
Figure 5: A dvantages o f fixed c o m p le te im p la n t prostheses (H o bkirk 2 0 0 3 ).
Figure 6: D isadvantages o f fixed c o m p le te im p la n t prostheses (H o bkirk 2 0 0 3 ).
Figure 7: Locator a tta c h m e n ts fo r im p la n t o v e rd e n tu re .
Figure 8: D o ld e r bar fo r m axillary tissue -im p la n t- su p p o rted o v e rd e n tu re .
Figure 9: D older b ar fo r tis s u e -im p la n t- su pp o rted m a n d ib u la r o v e rd e n tu re .
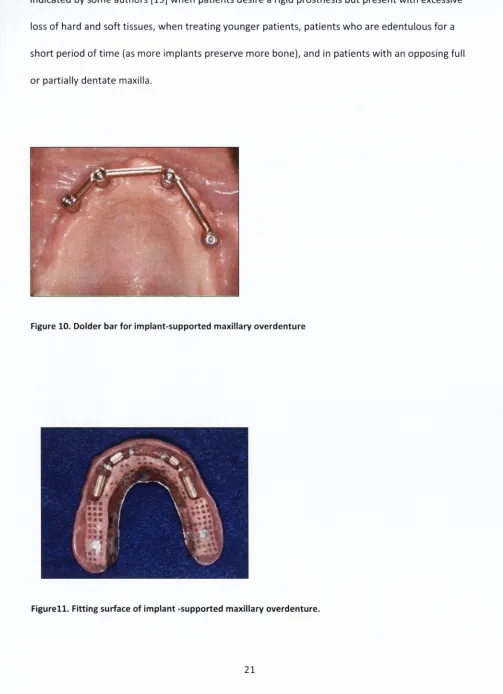
Figure 10: D older bar fo r im p la n t-s u p p o rte d m axillary o v e rd e n tu re .
Figure 11: Fitting surface o f im p la n t -su p po rted m axillary o v e rd e n tu re .
Figure 12: M a x illa n / im p la n t o v e rd e n tu re and m a n d ib u la r fixed prosthesis.
Figure 13: A dvantages o ff fixed /r e m o v a b le prostheses / M x /M n d (Strassburger 2 0 0 6 )
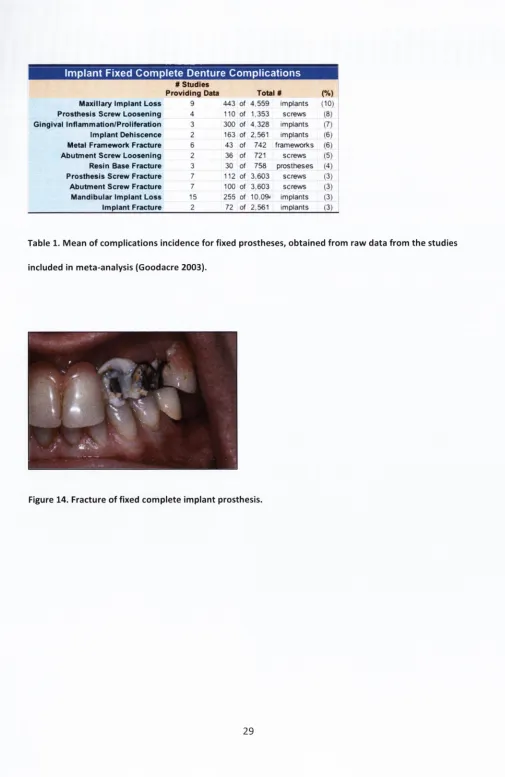
Figure 14: Fracture o f fixed c o m p le te im p la n t prosthesis.
Figure 15: Peri- im p la n t m ucositis a ffectin g a b u tm e n ts o f fixed im p la n t prosthesis.
Figure 16: Calculus on fittin g surface o f fixed im p la n t prosthesis.
Figure 17: Calculus and w e a r o f acrylic te e th on fixed im p la n t prosthesis
Figure 11: Gingival hyperplasia u n d e r D older b ar o f m axillary o v e rd e n tu re .
Figure 19: Fractured clips in im p la n t o v e rd e n tu re .
Figure 22: D ata reco rd ed fo r study pop u latio n .
Figure 23: Data reco rd ed in d atab ase fo r all im plants.
Figure 24: O H IP -1 4 q u estio n n aire.
Figure 25: P a tie n t Satisfaction Q u estio nn aire.
Figure 26: D ata reco rd ed fro m patien ts charts.
Figure 27: N u m b e r o f im plants placed each year.
Figure 28: Im plan ts by Prosthesis Type (p ercen tag es).
Figure 29: A ctual N u m b e r o f im plan ts supporting each prosthesis ty p e .
Figure 30: P ercentage o f im plan ts supporting each prosthesis typ e.
Figure 31: D istrib utio n o f im plan ts an ato m ically.
Figure 32: Types o f im plants.
Figure 33: Age p ro file o f p a tie n ts w h o received im plants.
Figure34: O ne w a y analysis o f overall satisfaction by fix e d /re m o v a b le
Figure35: Statistical S um m ary fo r overall satisfaction by fix e d /re m o v a b le
Figure 36: O ne w a y analysis o f aesthetics by fix e d /re m o v a b le
Figure 37: Statistical su m m ary fo r aesthetics by fix e d /re m o v a b le
Figure 38: O ne w a y analysis o f chew ing capacity by fix e d /re m o v a b le
Figure 39: Statistical su m m a ry fo r chew ing fu n c tio n by fix e d /re m o v a b le
Figure 40: O verall satisfaction by prosthesis ty p e (m axilla only)
Figure 41: Statistical su m m ary fo r overall satisfaction by prosthesis ty p e (m axilla only)
Figure 42: O ne w a y analysis o f p ro cedu re again by prosthesis ty p e (m axilla only)
Figure 4 3 . Statistical sum m ary fo r 'w illingness to have p ro ced u re again' by prosthesis typ e
Figure 4 4 . O ne w ay analysis o f tinne treatn nen t to o k by prosthesis ty p e (nnaxilla only)
Figure 4 5 . Statistical sum m ary o f tim e tr e a tm e n t to o k by prosthesis ty p e (m axilla only
Figure 4 6 . O ne w a y analysis o f A esthetics by prosthesis ty p e (m axilla only)
F ig ure47. Statistical su m m ary fo r A esthetics by prosthesis ty p e (m axilla only)
Figure 4 8 . O n e w a y analysis o f psychological d isco m fo rt by fix e d /re m o v a b le
Figure 4 9 . Statistical S um m ary fo r psychological by fix e d /re m o v a b le
Figure 5 0 . O n e w a y analysis o f psychological disability by fix e d /re m o v a b le
[image:28.524.15.514.6.761.2]List of Tables
T a b le l. M e a n o f com plications incidence fo r fixed prostheses, o b ta in e d fro m ra w data fro m
th e studies included in m eta-analysis (G oodacre 2 0 0 3 ).
Table 2. M e a n o f com plications incidence fo r im p la n t o v e rd e n tu re s , o b ta in e d fro m raw data
fro m th e studies included in m eta-analysis (G oodacre 2 0 0 3 ).
Table 3. P a tie n t satisfaction su btotal scores (percentages)
Table 4. P a tie n t satisfaction su btotal scores (p ercen tag es)
Table 5. M a x illa ry s u bg ro u p :P atien t satisfaction subtotal scores (percentages)
Table 6. M a x illa ry subgroup: p a tie n t satisfaction su btotal scores (p ercentages)
Table 7. O H IP su btotal scores (p ercen tag es)
Table 8. M a x illa ry group: OHIP su btotal scores (percentages)
Table 9. O v e rd e n tu re Com plications
[image:30.524.17.521.22.757.2]I
> ^ : r « ' K ^ i ' t^ . . ■ W ! f «
m
. • c / T S i R ^ K - ' .
i f - * ]
^
.jBrtjir
. ■ ■ ■ j . ’ — . , ■ I ■ r . i . -f t ' >.
^ ■ J j ^ W - T "
_
* 3 ^ .» ■ * . J V ^ ' 3
T'. : ■ . - " ■ ^ ■
i ' j
■ M u |i I . i t ' ^ 1 1
-■ -■ V -■ V
Chapter 1: Introduction
E dentulism , according to W o rld H ealth O rgan izatio n (W H O ) [1] c riteria, is considered a physical
im p a irm e n t since im p o rta n t body parts have been lost. M a n y ed e n tu lo u s patien ts e xp erien ce
im p a ire d ab ility to p erfo rm essential life tasks, n a m e ly speaking and eating. D ental im plan ts are
accep ted as a successful a lte rn a tiv e to co nven tio nal fixed and re m o v a b le prostheses and have
been d e m o n s tra te d to be p red ictab le and m o d e ra te ly tro u b le -fre e fo r th e tr e a tm e n t o f
e d e n tu lis m .
O ver th re e decades ago, th e first articles on th e use o f tita n iu m o ral im plants in hum ans w/ere
published [2]. Today, o v e r 8 0 0 0 publications on o ral im plants in hum ans are fo u nd in th e
lite ra tu re . How/ever, fe w e r th an 2% o f th ese deal w ith p a tie n t-c e n tre d o utcom es o f im p la n t
d e n tis try . T he consensus re p o rt o f th e first European W o rk s h o p on P erio d o ntolo gy [3] included
re c o m m e n d a tio n s th a t p a tie n t- c en tred o utcom es should be reco rd ed during th e e valu atio n
period. This claim has been re ite ra te d in a re p o rt based on th e proceedings o f th e T o ro n to
Sym posium ( 1 9 9 8 ) , which concluded th a t p a tie n t satisfaction o u tc o m e m easures should be
included in fu tu re im plan t success criteria [4] and again by Lang a t th e 2 0 0 2 European W o rksh o p
on P e rio d o n to lo g y .[5]
M o s t researchers w o u ld now agree th a t tr e a tm e n t ev a lu a tio n should be based on th e p atien t's
o w n ratings o f tr e a tm e n t success as w ell as tra d itio n a l clinical p a ra m e ters . T he assessm ent o f th e
p a tie n t perspective provides a scaffold fo r im p ro v e m e n ts in h ealth and d e n ta l care, and also
supports th e co ncep tu al ap proach o f p a tie n t -c e n tre d care.
For m o re th an o n e hundred years, only o ne tr e a tm e n t has been availab le fo r th e tr e a tm e n t of
e d e n tu lis m -co n ventio n al d en tu res. These rely on th e fo rm o f th e rem ain in g bony ridge fo r
su p p o rt and re te n tio n , but even w h e n th e d e n tu re s are ju d g ed to be excellen t, m an y ed entulo us
Modern prosthodontics has developed a sophisticated range of possible treatments and
materials. Today there are three prosthodontic tools available to restore an edentulous arch;
conventional denture, an implant- retained and tissue -supported removable overdenture, or an
implant-supported and retained fixed prosthesis. Unfortunately, the majority o f studies
comparing these types of prostheses have not used validated instruments which makes
comparisons less valid and meaningful.
Objectives of Study
While the literature reports a high level of general satisfaction w ith both implant overdentures
[7-9] and complete fixed implant prostheses [10-12], few surveys have been conducted which
compare patient satisfaction and oral health related quality of life fo r the tw o treatm ent
modalities. Firm criteria are lacking on which parameters are im portant in deciding which
prosthesis is appropriate and the literature has mixed reports on which type o f prosthesis is more
satisfactory.
General objectives of this study will be to assess complete implant fixed prostheses and
removable implant prostheses (overdentures), whether they be maxillary or mandibular, in terms
of patient satisfaction and oral health related quality of life. For example, do patients with a 'fixed
prosthesis' have less psychological disability, functional lim itation or social disability than those
w ith a 'removable prosthesis' ?.
More specific aims will be to report on patient satisfaction in terms o f (1) patient perceptions of
selected technical aspects of treatm ent outcome, (chewing function, comfort, speech,
cleansability ) (2) patient perceptions of treatm ent experience, (3) incidence o f complications, and
o f oral h ealth re la te d quality o f life are m o re im p o rta n t in d e te rm in in g p a tie n ts ' overall
p e rc e p tio n o f o ral health related quality o f life.
Previous studies have co m p ared o v e rd e n tu re s su pp o rted by tw o im plants (sim ple o v e rd e n tu re s )
w ith fixed c o m p le te dentures. T he profile o f a p a tie n t w h o receives o ne o r tw o im plants to
stabilize th e ir d e n tu re is considerably d iffe re n t fro m a p a tie n t w h o is generally younger, has m o re
availab le bone and is p o te n tia lly suitable fo r a fixed prosthesis o r a ' com p lex' o v e rd e n tu re . It is
,th e re fo r e in a p p ro p r ia te to c o m p a re a fixed prosthesis to a 'sim ple' o v e rd e n tu re , as w ith o u t a
consid erab le g ra ftin g p rocedure, a fixed o ptio n w o u ld rarely be an o ptio n fo r a p a tie n t w h o
received a 'sim ple' o v e rd e n tu re . For this reason a m in im u m o f fo u r im plants w o u ld be req u ired
Chapter 2: Literature Review
Outcome Measures:
Implant Survival versus Success:
W ith d e n ta l im p la n ts suggested to be th e m in im u m sta n d ard o f ca re fo r th e e d e n tu lo u s p a tie n ts [13 ]
and w ith th e g ro w in g use o f ro o t fo rm endosseous im p la n ts fo r p a rtia lly d e n ta te p a tie n ts , it is
im p e ra tiv e to establish success c rite ria fo r im p la n t system s, and fo r im p la n ts to be te s te d in w ell
c o n tro lle d clinical trials. This, a b o v e all, is to p ro te c t p a tie n ts and p res erve th e ir rig ht to in fo rm e d
con sent as to th e risks and b e n e fits o f any p ro po sed tr e a tm e n t [1 4 ] .
The clinical crite rio n m o st fre q u e n tly re p o rte d is th e survival ra te , o r w h e th e r th e im p la n t is still
physically in th e m o u th . P ro p on en ts o f this m e th o d say it pro vides th e m o st a c c u ra te re p re s e n ta tio n
o f th e d ata; critics arg u e th a t im p la n ts th a t should be re m o v e d becau se o f pain, disease o r th e
in a b ility to be re s to re d m ay be m a in ta in e d and w ro n g fu lly re p o rte d as successful.
A u niversal d e fin itio n fo r im p la n t success versus survival has b e e n d iffic u lt to estab lish , o w in g t o th e
u n c le ar p red ictive m easures o f c o n v e n tio n a l p e rio d o n ta l m e a s u re m e n t te c h n iq u e s (fo r e x a m p le ,
p e rio d o n ta l p ro bin g o f im p lants). S u rro g ate m easures such as p ro b in g aro u n d im p la n ts o n ly m e as u re
local in fla m m a tio n , w h ich m ay o r m a y n o t re la te to im p la n t o u tc o m e s [1 5 ] . Equally im p o rta n t, a study
Success versus Survival Criteria:
W h ile c rite ria fo r im p la n t success have been p u b lis h e d [1 7 ], th e ir fo cu s o fte n has been im p la n t
s y s te m -s p e c ific , w h ic h has re s u lte d in g re a te r em p h a sis on im p la n t su rviva l ra th e r th a n success.
Success c rite ria fo r e n d o ste a l im p la n ts have p re v io u s ly been re p o rte d by several a u th o rs. In 1975, th e
Sw edish N a tio n al Board o f H ealth and W e lfa re m a d e o n e o f th e firs t a tte m p ts to e v a lu a te th e clin ica l
p e rfo rm a n c e o f o sse o lnte g ra te d o ra l im p la n ts . P e rio d o n ta l (p la q u e in d e x , g in g iva l index, and p o c k e t
d e p th s ), p ro s th e tic and ra d io g ra p h ic p a ra m e te rs (absence o f p e ri-lm p la n t ra d io lu ce n c y ), to g e th e r
w ith th e p a tie n t's o p in io n on th e tr e a tm e n t, w e re used. A lb re k tss o n p ro p o se d s tric te r c rite ria w h ic h
have been g e n e ra lly accepted (fig u re 1) [18].
Criteria fo r Im p lan t Success
• An individual unattached im plant is im m obile when tested clinically,
• The radio gra ph does not demonstrate any evidence of periim plant radiolucency.
• Vertical bone loss is less than 0.2 m m annu ally after the first year of service of the im plant.
• Individual im plant performance is characterized by an absence of persistent or irreversible signs and symptoms such as pain, infections, neuropathies, paresthesia, or violation of the mandibular canal.
• In the context of the foregoing, success rates of 85% at the end of a 5-year observation period and 80% at the end of a 10-year period are m inim um criteria for success.
Figure 1 .Implant Success Criteria proposed by Albrektsson 1986
C o n v e n tio n a l p e rio d o n ta l indices w e re n o t in clu d e d , because th e y w e re n o t co n sid e re d to be re la te d
to im p la n t success, and th is o p in io n was s u p p o rte d by S m ith and Zarb [14] w h o did n o t co n sid e r it
necessary to in clu d e any m easure o f m ucosal h e a lth in th e ir p ro p o se d c rite ria fo r im p la n t success.
S m ith and Zarb also suggested th a t p a tie n t c o m fo rt, sulcus d e p th , g in g iva l status, dam age to a d ja c e n t
[image:38.524.24.509.230.768.2]design o f th e im plant and th erefore should be considered independently. Mische suggests th a t
Im plant survival by itself is not an acceptable criterion to evaluate an im plant system and must include
the restoration[19]. Hence im plant survival and associated prosthesis survival rates need to be
evaluated to g eth er because th e most im portant com ponent to the p atien t is th e restoration.
In 1988, at the second NIH Consensus Conference [20] it was concluded th a t d ifferen t success criteria
should be applied to d ifferen t im plant systems. It was proposed th a t probing depths be excluded, as
they may be correlated to the thickness of the m ucoperiosteum and th e re fo re may not be related to
im plant success or failure. At the 1st European W orkshop on Periodontology, consensus agreed that
an absence of mobility, an average radiographic marginal bone loss o f less than 1.5 mm during the first
year o f function and less than 0.2 mm annually th e re a fte r, and absence o f pain a n d /o r paresthesia,
w ere to be considered success criteria for im plants[3]. It was also proposed th a t probing depths
related to a fixed reference point and bleeding on probing should be evaluated. Periodontal
param eters w ere introduced to b e tte r describe the condition of peri-im plant tissues to facilitate the
identification of failing implants clinically [3].
Patient centred-outcomes:
In th e lite ra tu re w h ich addresses im p la n t success p a tie n t c e n tre d -o u tc o m e s a re usually n o t
re p o rte d and y e t, m ay p resen t m a jo r aspects o f th e im p la n t success fo r th e p a tie n t. Since som e o f
th e m o re im p o rta n t criteria fo r assessing th e q u ality o f im p la n t restoratio n s are subjective, it is
im p e ra tiv e to in q u ire ab o u t th e p a tie n t's opin io n , which m ay d iffe r fro m th a t o f th e clinician, so
as to ensure p a tie n t satisfaction w ith th e final o u tc o m e . In d eed p ro sth etic tr e a tm e n t m ay be
tech n ically co rre c t and a t th e sam e tim e a clinical fa ilu re if th e p a tie n t is unsatisfied w ith th e
Im p la n t survival, prosthesis lo ngevity, and th e fre q u e n c y o f com plications are regarded as th e
m ost significant outcom es to th e clinician. On th e o th e r hand social and psychological im p a c t o f
tr e a tm e n t, cost effectiveness, b e n e fit and u tility a re m o re im p o rta n t fro m th e p atien ts'
perspective [21, 2 2 ] .
A m o re co m p reh ensive e v alu atio n o f p ro sth od o n tic o utcom es w as proposed by A nderson in th e
late 1 9 9 0 s [2 3 ]. This divides pro sth etic o utcom es into fo u r d istinct categories 1: biologic and
physiologic p a ra m e ters (h ealth o f oral structures, chew ing ability, n u tritio n a l status, aesthetics);
2: longevity and survival (o f te e th , im plants, restorations); 3: psychosocial p a ra m e te rs (tre a tm e n t
satisfaction, self e s te e m , body im age, q uality o f life) and 4: econom ic p a ra m e ters (cost o f
fa b ric a tio n and m a in te n a n c e , in d irect cost). In re c e n t years th e re has been a significant increase
in in te re s t in assessing th e psychosocial o utcom es o f oral h ealth .
In a system atic re v ie w o f th e lite ra tu re Strassburger e t al [24] found th a t th e use o f broad
questions o f g eneral satisfaction w e re g enerally su p p le m e n te d w ith m o re specific questions on
ch ew ing /s p e e c h fu n ctio n . These factors w e re proved to be th e m ost closely c o rre late d w ith
o verall satisfaction , at least in th e case o f m a n d ib u la r fixed im p la n t prostheses as w as found by
A w ad and Feine [25]. As broad , non -specific questions te n d to cause a large n u m b e r o f false
positives, this fo rm o f questions should always be s u p p le m e n te d w ith m o re specific
ite m s [2 6 ].T h is has been re ite ra te d by Strassburger w h o stated th a t 'sim ply inquiring into th e
g eneral satisfaction o f p atien ts w ith d en tal prostheses o fte n does n o t suffice w h e n assessing th e
im p a c t o f d en tal tr e a tm e n t on p a tie n ts '[2 7 ]. D e ta ile d questions on factors such as co m fo rt,
aesthetics, ease o f cleaning and chew ing fu n ctio n w ill give an insight into which aspects can be
Patient Satisfaction
In a re v ie w o f p a tie n t satisfaction w ith all ty p e o f prostheses fro m 1 9 6 0 -2 0 0 3 , Strassburger [27]
re p o rte d a g eneral satisfaction ra te o f 83% . This high g eneral satisfaction rate m ay be d ue to th e
fa c t th a t g eneral questions yield m o re positive responses th a n n a rro w ly focused ones. T he criteria
fo r assessm ent o f p a tie n t satisfaction in this e a rly period w e re c o n fin e d to basic clinical factors
such as fit, chew ing a b ility or ju s t general satisfaction. A m o re d e ta ile d study w as carried o u t by
Sm ith and Sheiham in 1 9 7 9 [2 8 ]. In this study 2 5 4 p atien ts, 75% o f w h o m w e re e d e n tu lo u s , w e re
q u estio n ed on th e ir satisfaction w ith th e ir c o m p le te d entures. T w e n ty -fiv e p e rc e n t re p o rte d pain
w h en eatin g and fo rty -o n e p e rc e n t n eeded m o re tim e w h e n c h ew ing as a resu lt o f becom ing
ed en tu lo u s. As a result, p atien ts re p o rte d (psychological) d is c o m fo rt w h e n e a tin g in com pany.
For th e first tim e th e relatio n sh ip b e tw e e n unsatisfactory prostheses and daily activites becam e
e v id e n t.
In a re v ie w o f th e lite ra tu re ev a lu a tin g th e relatio n sh ip b e tw e e n p a tie n ts ' opinions o f th e ir
de n tu re s and clinical assessments o f th e prostheses, no significant relatio n sh ip w as fo u n d . The
authors concluded th a t clinical assessments o f prostheses are n o t valid p redictors o f patients
s a tisfaction [29]. It w o u ld a p p e a r th a t p atien ts' satisfaction w ith th e ir d entures is likely to be
re la te d to th e ir o w n percep tio n s o f th e ir ab ility to p e rfo rm oral fu nctions successfully.
Oral Health Related Quality of Life
O ral h ealth is d e fin e d as fre e d o m fro m chronic facial pain; oral and pharyngeal cancers; oral soft
tissue lesions; b irth d efects such as c le ft lip and palate; and o th e r diseases a ffe c tin g th e oral,
Q u a lity o f Life is d efined as an individual's percep tio n o f his or h er position in life, in th e co n te x t of
th e c u ltu re and value systems in w hich th e y live, and in relatio n to th e ir goals, exp ectation s and
concerns [3 1 ],
Oral H ealth -r e la te d QOL is d e fin e d as an individual's assessm ent o f h o w th e fo llo w ing a ffe c t his
or h e r w ell being: functional factors, psychological factors, social factors, and exp erien ce o f
p a in /d is c o m fo rt in relation to oro facial concerns [32],
T h e re fo re , w e see th a t OHRQOL is a m o re co m p reh ensive m u ltid im en sio n al e v alu atio n o f th e
consequences o f prosthetic re h a b ilita tio n [33]. W h ile n um ero us o ra l- specific m easures have
d e v e lo p e d o v e r th e last 20 years, th e Oral H ealth Im pact P rofile (O HIP) has e m e rg e d as a
p o w e rfu l to o l in th e assessment o f Oral health related q u ality o f life (O HQ OL) [24] An existing
m o d el o f o ral h ealth [34] was used by Locker to id en tify co ncep tu al d om ains in th e hierarchy o f
social im pact. In this m odel disease can lead to im p a irm e n t, d e fin e d as any an ato m ical loss ( ie,
loss o f a to o th ). Im p a irm e n t m ay lead to fu n ctio n al lim ita tio n , fo r e x am p le d ifficu lty in m aking
p a rtic u la r sounds. This m ay lead to physical, psychological o r social disability, described by Locker
as 'an y lim ita tio n in o r th e lack o f ab ility to p e rfo rm activities o f daily living'.
Impairment
Functional limitation U Discomfort and pain
Physical Psychological
Social
Handicap
The OHIP questionnaire encompasses seven conceptual domains of impact: functional lim itation,
(for example, difficulty chewing foods), physical pain (for example ,toothache), psychological
discomfort (for example self consciousness), physical disability (for example, avoiding foods)
psychological disability (for example, being embarrassed), social disability (for example , difficulty
doing jobs), and handicap (for exam ple, being totally unable to function).The OHIP has proved its
high ability to discriminate among different population groups[35] The use of OHQOL
questionnaires provides a patient perspective on the outcome o f prosthodontic treatments and
may help evaluate the benefits of the various treatm ent protocols.
Review of studies relating to Oral Health Related Quality of Life
Several studies have shown that oral function is significantly improved in edentulous patients
after implant treatment. In one study patients considered the osseointegrated prostheses to be
part of their bodies, leading to an obvious improvement in the ir life [36]. Furthermore ,
significant improvements have not been limited to the teeth, but include the face, mouth, and
overall self-image [37],
In 2006, Naito et al. [30] carried out a systematic review to investigate a link between oral health
status and health related quality o f life. A total of 1726 articles were reviewed and only seven
were deemed suitable for analysis. Four of the seven studies indicated a relationship between
oral health status and health related quality of life. The author concluded that providing
edentulous patients w ith implant supported full dentures contributed to improved health related
quality of life.
Treatment of the edentulous maxilla:
A systematic review o f the literature investigating the influence o f implant and conventional
h undred and fo u rte e n studies published b e tw e e n 1 9 6 0 and 2 0 0 3 w e re re v ie w e d and th e re w e re
38 studies reaching evidence level I o r II.( Agency fo r H ealth Care Policy and Research )[3 8 ].
T w o random ised co ntrolled trials w e re in d en tified th a t d e a lt w ith tr e a tm e n t o f th e ed entulo us
m axilla. C om pared to th e p re -tre a tm e n t evalu atio n w ith co nven tio nal dentures, o ne study
show ed increased satisfaction a fte r insertion o f im p la n t su pp o rted re m o v a b le o verd entures.
H o w e v e r th e re was no d iffe re n c e b e tw e e n d e n tu re s w ith and w ith o u t palatal coverage [39]
Heydecke e t a l . [40] carried o u t a w ith in -subject com parison o f m axillary fixed and re m o v a b le
im p la n t prostheses. R em ovable long bar o v e rd e n tu re s based on fo u r to six im plants received
significantly hig h er ratings o f g eneral satisfaction th a n fixed prostheses. P atients rated th e ir a b ility
to speak and ease o f cleaning significantly b e tte r w ith re m o v a b le prostheses. Nine p atien ts chose
to keep th e re m o v a b le prosthesis and fo u r p re fe rre d to keep th e fixed prosthesis.
Treatm ent of the edentulous mandible:
A w ad e t al .carried o u t tw o random ised co ntro lled trials co m p arin g m a n d ib u la r im plan t
o v e rd e n tu re s and conven tio nal d entures in tw o p a tie n t p opulations, m idd le aged (3 5 -6 5 ) and
senior (6 5 -7 5 ) [4 1 , 4 2 ]. In th e yo un g er group, th e y fo u nd th a t OHIP scores w e re significantly lo w e r
(b e tte r) in th e im p la n t group th a n in th e group restored w ith co n v e n tio n a l c o m p le te d entures.
H o w e v e r in th e m o re senior group, w h ile OHIP scores w e re lo w e r in th e im p la n t group in each o f
th e seven dom ains, th e e ffe c t was only significant in th e physical d om ain . T he authors concluded
th a t th e d ifferen ces b e tw e e n th ese tw o RCTs w e re likely d ue to th e fa c t th a t th e subjects in senior
study w e re less likely to be engaging in th e activities assessed in th e OHIP.
Sim ilar findings have been re p o rte d by Allen e t al [43], w h o fo u nd th a t OHIP scores o f previous
c o m p le te d e n tu re w e a re rs w h o req u ested , but did not receive im p la n t tr e a tm e n t, did not change,
t r e a t m e n t ( i m p l a n t o v e r d e n t u r e ) . This su g g e s ts t h a t choice m a y h a v e a s tr o n g in flu en ce o n oral
h ea lth r e la te d quality o f life. W hile m a n y p a t i e n t s t o l e r a t e c o n v e n tio n a l c o m p l e t e d e n t u r e s ,
p a tie n t satisfactio n a n d oral h e a lth re la te d quality o f life im p ro v e s significantly if t h e m a n d ib u la r
d e n t u r e is s u p p o r t e d by as fe w as t w o im p la n ts [25, 29, 43, 4 4 ] .
B oum a , B o errig ter e t al. c o m p a r e d t h r e e g r o u p s (Im plant r e t a i n e d o v e r d e n t u r e , c o m p l e t e
d e n t u r e , p r e - p r o s t h e t i c s u r g e r y / c o m p l e t e d e n t u r e ) for th e i r e ffe c ts o n fu n c tio n a l ability (chewing,
speaking, etc), p a t i e n t satisfaction, a n d quality o f life (psychosocial functioning) [45], Twelve
m o n t h s a f t e r t r e a t m e n t , p a tie n ts in all t h r e e g r o u p s e x p e r ie n c e d f e w e r restric tio n s in t h e i r social
activities a n d h a d f e w e r psychological p r o b le m s b e c a u s e o f t h e i r c o m p l e t e d e n t u r e s . W hile it w as
of no su rp rise, t h a t t h e im p la n t r e t a in e d o v e r d e n t u r e g ro u p im p ro v e d significantly in th e ir
psychosocial functio n in g , it w a s r e m a r k a b le t h a t a similar effe c t w a s s h o w n in t h e p re - p r o s th e tic
s u rg ery g ro u p . The a u t h o r s q u e s tio n w h e t h e r t h e positive resu lts in all 3 g r o u p s could be
a t t r i b u t e d t o t h e p a t i e n t 's k n o w le d g e t h a t t h e y a re particip atin g in a trial ( t h e so called H a w th o rn
Effect).This w a s d is p u te d , given t h e fact t h a t t h e s e findings w e r e s ta b le o v e r t i m e a n d t h a t t h e
s a m e p a tie n ts did d i f f e r e n tia te b e t w e e n p a t i e n t satisfactio n an d fu n ctio n al s y m p to m s . The d e n ta l
im p la n t g r o u p r e p o r t e d m u ch b e t t e r functional ability th a n t h e p r e - p r o s t h e t i c su rg ery group, and
t h e l a tte r w a s m u c h b e t t e r t h a n t h e c o m p le te d e n t u r e s alone.
A m u lti-c e n tre r a n d o m iz e d c o n tro lle d trial carried o u t by t h e s a m e g ro u p , c o m p a r e d im plant
o v e r d e n t u r e s w ith c o n v e n tio n a l d e n t u r e s in t e r m s o f d e n t u r e satisfaction[46] It w a s f o u n d t h a t
g e n e ra l satisfaction r a t e an d t h r e e o u t o f five f a c to rs s h o w e d significantly b e t t e r s c o re s for t h e
g ro u p t r e a t e d w ith im p lan ts t h a n fo r t h e c o n tro l-g ro u p . It w a s striking t h a t 64% o f t h e c o m p le te
d e n t u r e g r o u p w e r e satisfied w ith t h e g e n e ra l satisfaction. Again it is s u g g e s te d t h a t t h e r e m ight
b e a ca re effe c t in t h e co n tro l g r o u p ie p a tie n ts a re t r e a t e d w ith a lot o f p a t i e n c e and
T h e re fo re it is a p p a re n t th a t im p ro v e m e n ts in q u ality o f life (psychosocial fu n ctio n in g ) should be
in te rp re te d w ith caution.
Oral Health Impact Profile
Im p ro v e m e n t in OHRQOL as m easu red w ith OHIP scores has readily been d o c u m e n te d w ith th e
provision o f im p la n t supported versus co nven tio nal prostheses (no im plants) [2 9 ]. H o w e v e r little
is know n a b o u t th e influence o f d iffe re n t types o f im p la n t prostheses on OHRQOL .
The OHIP evalu ates th e consequences o f oral conditions across dim ensions o f fun ctio n al
lim ita tio n , physical pain, psychological d iscom fort, physical disability, social disability and
handicap. T he dim ensions w e re in te n d e d to re fle c t a h ierarchy o f increasingly disruptive im pacts
on people's lives. For instance, th e fu n ctio n al lim ita tio n questions c ap tu re effects th a t w ould be
p e rc e p tib le principally to th e individual, such as "H ave you had tro u b le pronouncing any words
because o f problem s w ith yo ur im p la n t prosthesis?" Q uestions in th e disability d o m a in re fe r to
factors which im p a c t on everyday activities such as "H ave you had d ifficu lty doing y o u r usual jobs
because o f pro blem s w ith yo ur im p la n t prosthesis?",w hile handicap rep resen ts th e e x te n t of
d ifficu lty caused by oral health, such as "H ave you fe lt th a t life in g eneral w as less satisfying
because o f problem s w ith yo ur im p la n t prosthesis?"
W h ile th e OHIP is in te n d e d to provide c o m p reh ensive d ata a b o u t p erceptions o f im pact on w ell
being, th e full 4 9 -ite m version is n o t practical in a clinical setting d ue to its length. This led to th e
d e v e lo p m e n t by Slade o f a s h orter fo rm , th e O H IP -1 4 [4 7 ], This fo rm consists o f 14 item s, tw o
fro m each subscale, selected because th e y have been show n to be th e m ost fre q u e n tly rep o rted
Fixed restoration of the complete edentulous arch
Im p la n t su pp o rted fixed c o m p le te d entures w e re th e first prosthesis to be used successfully w ith
im plants and th e re fo re have th e longest record o f clinical e x p e rie n c e and research [4 8 ]. T he
psychological advantage o f a fixed re s to ra tio n is o f great b e n e fit, and p atien ts o fte n fe e l th e
im p la n t te e th are " b e tte r th a n m y o w n te e th " A p o te n tia l disad van tag e is th a t th e im plan ts m ust
be precisely placed, particularly in th e highly aesth etic a n te rio r zone.
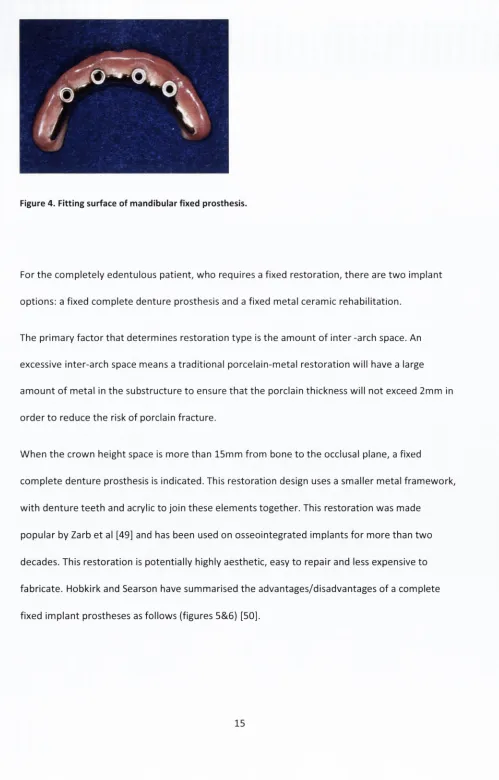
Figure 4. Fitting surface of mandibular fixed prosthesis.
For th e c o m p le te ly ed entulo us p a tie n t, w h o requires a fixed re s to ra tio n , th e re are tw o im plan t
options; a fixed c o m p le te d e n tu re prosthesis and a fixed m etal ceram ic reh a b ilita tio n .
T he p rim a ry fa c to r th a t d e te rm in e s resto ratio n ty p e is th e a m o u n t o f in te r -arch space. An
excessive in te r-a rc h space m eans a tra d itio n a l p o rc e la in -m e ta l re s to ra tio n w ill have a large
a m o u n t o f m e ta l in th e substructure to ensure th a t th e porclain thickness w ill not exceed 2 m m in
o rd e r to reduce th e risk o f porclain fra c tu re .
W h e n th e cro w n heig h t space is m o re th a n 1 5 m m fro m bone to th e occlusal plane, a fixed
c o m p le te d e n tu re prosthesis is in dicated. This re s to ra tio n design uses a sm aller m e ta l fra m e w o rk ,
w ith d e n tu re te e th and acrylic to join th ese e le m e n ts to g e th e r. This re s to ra tio n w as m ade
p o p u la r by Zarb e t al [49] and has been used on o s seoin teg rated im plants fo r m o re th an tw o
decades. This re s to ra tio n is p o te n tia lly highly aesth etic, easy to re p a ir and less expensive to
fa b ric a te . H obkirk and Searson have sum m arised th e a d vantages/d isad vantages o f a co m p lete
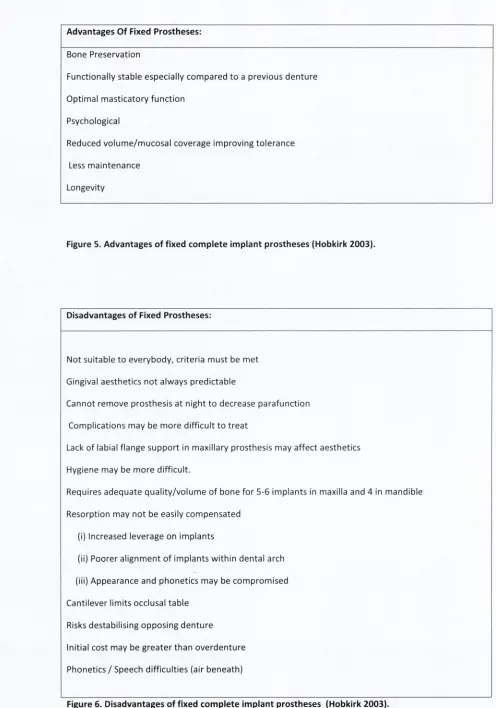
[image:48.524.20.519.21.801.2]Advantages O f Fixed Prostheses:
Bone Preservation
Functionally stable especially compared to a previous denture
Optimal masticatory function
Psychological
Reduced volume/mucosal coverage improving tolerance
Less maintenance
[image:49.524.15.511.18.726.2]Longevity
Figure 5. Advantages of fixed complete Im plant prostheses (Hobkirk 2003).
Disadvantages of Fixed Prostheses:
Not suitable to everybody, criteria must be met
Gingival aesthetics not always predictable
Cannot remove prosthesis at night to decrease parafunction
Complications may be more difficult to treat
Lack of labial flange support in maxillary prosthesis may affect aesthetics
Hygiene may be more difficult.
Requires adequate quality/volum e of bone for 5-6 implants in maxilla and 4 in mandible
Resorption may not be easily compensated
(i) Increased leverage on implants
(ii) Poorer alignment o f implants w ithin dental arch
(iii) Appearance and phonetics may be compromised
Cantilever limits occlusal table
Risks destabilising opposing denture
Initial cost may be greater than overdenture
Phonetics / Speech difficulties (air beneath)
Number of Implants:
Davis et al., in 1988 examined th e effect o f varying th e num ber o f supporting abutm ents fro m a
m etal fra m e w o rk stress analysis perspective and concluded th a t successful results are best
achieved using fo u r o r five im plants [51]. A ten year study conducted by Branemark found high
success rates fo r both maxilla and m andible w/hen both 4 and 6 im plants w ere used [52],
Maxilla;
Authors and researches vary in th e ir recom m endation fo r between 4 and 6 im plants. Mische
recom m ends between 7 and 10 im plants to maximize the anterior-poste rior spread, particularly
when bone quality is poor o r occlusal forces are high. Six im plants are often considered the
m inim um fo r use in the maxilla, as the average im plant loss is greater in th e maxilla due to many
factors[53], such as:
• poorer bone quality and density compared to m andible
• placem ent challenges due to pattern o f bone resorpion
• unfavorable loading angle as te e th w ill be usually facially inclined and th e re fo re the
im plant w ill not be loaded along its vertical axis.
• th e presence o f vital structures (mainly th e maxillary antrum )
A m o re re c e n t te c h n iq u e has evo lved , ad vocated by Dr Paulo M a o lo , w h e re b y fo u r im p la n ts are
placed to support th e fixed prosthesis. T w o are placed p osteriorly, o n e on each side and tw o
placed a n te rio rly n e a r th e c e n te r o f th e arch. T he tw o p o s te rio r im plan ts a re angled w ith th e ir
apices m esially to avoid th e sinus (to avoid need fo r sinus lift and g ra ftin g ), th e to p o f th e im p la n t
is thus distally exposed, reducing th e length o f c a n tile v e r (The All on 4 te c h n iq u e ). M o re research
is req u ired b efo re this te c h n iq u e can be w id e ly accepted.
Mandible:
Up to 6 im plants m ay be placed in th e in tra -fo ra m in a l region o f th e m a n d ib le. A five y e a r study by
Eliason e t al., in 2 0 0 0 fo u nd a survival rate o f 98% o f m a n d ib u la r fixed c o m p le te d e n tu re s
su pp o rted by 4 im plants only [54].
If s h o rte r im plants are req u ired (less th an 1 0 m m ), th e n it is re c o m m en d e d to place 5 o r 6 if
possible [51] .B ran em ark in tro d u ced a design th a t uses 3 im plants in th e m a n d ib le th a t are 5 m m
in d ia m e te r [52] .The All on 4 te c h n iq u e has also been suggested fo r th e m a n d ib le w ith p osterio r
im p la n t apices located m esially to avoid th e m e n ta l fo ra m e n .
Removable Prosthesis
T he re m o v a b le im p la n t re s to ra tio n has becom e o ne o f th e m ost successful applications o f im p la n t
d e n tis try o ver th e last tw o decades. Today's pop u latio n is living lo n g er and th e y are much
h e a lth ie r th an in th e past, b u t ed en tu lism is still very p re v a le n t.
The p rim ary aim o f an im p la n t o v e rd e n tu re is to add to th e stability and re te n tio n o f a rem ovab le
prosthesis. T h e re fo re th e p a tie n t usually presents com plaining o f an existing prosthesis th a t lacks
be the "first choice standard o f care" for the edentulous mandible. Nonetheless not all authors
agree with this assumption. In a review of the literature Fitzpatrick [55] stated that there was no
definitive proof that an implant overdenture was the superior form of restoration for the
edentulous mandible. He stated that "Clinicians should avoid applying one universal treatm ent
intervention. Choice o f treatm ent modality should evaluate both dentist- and patient-mediated
factors, including treatm ent and maintenance costs"
Due the huge variety of designs available it is helpful to have a system of nomenclature that
allows description and categorization of the various prostheses. Implant overdentures can be
classified according to the superstructure attached to the implant from which the overdenture
obtains support and retention. One can differentiate between :
Tissue-supported Overdenture: the retentive mechanism is a magnet or ball attachment and the
denture rests on the mucosal tissues. The attachments ensure retention only during lateral and
extrusive movements (figure 7).
Figure 7. Locator attachm ents fo r implant overdenture.
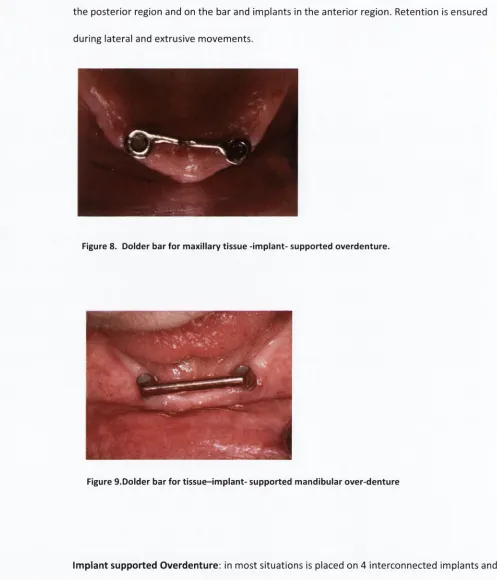
Tissue-implant-supported Overdenture: retention is provided via a bar connecting two implants
the posterior region and on the bar and implants in the anterior region. Retention is ensured
during lateral and extrusive movements.
Figure 9.Dolder bar for tissue-im plant- supported mandibular over-denture
Implant supported Overdenture:
in most situations is placed on 4 interconnected implants and
the denture rests primarily on the superstructure, w/hile the mucosal bearing areas are minimally
loaded during occlusal function.
Indications for the tissue implant supported overdenture may include the maladaptive or
[image:53.524.9.506.39.619.2]p a t i e n t s desiring a m o r e s ta b le m a n d ib u la r d e n t u r e [56]. Im plant s u p p o r t e d o v e r d e n t u r e s a re
in d ic a te d by s o m e a u t h o r s [19] w h e n p a tie n ts d e s ire a rigid p ro s th e s is b u t p r e s e n t with excessive
loss o f h a rd an d so ft tissues, w h e n t r e a t i n g y o u n g e r p a tie n ts , p a t i e n t s w h o a r e e d e n t u l o u s fo r a
s h o r t p erio d o f tim e (as m o r e im p la n ts p r e s e r v e m o r e b o n e), an d in p a t i e n t s w ith an o p p o s in g full
o r partially d e n t a t e maxilla.
Figure 10. D older bar for im p la n t-su p p o rted m axillary o v e r d e n tu r e
[image:54.524.9.512.75.769.2]Figure 12. M axillary im plant overdenture and mandibular fixed prosthesis.
Choice of Prosthesis
Several designs o f prosthesis can be used to re s to re th e e d e n tu lo u s p a tie n t. An o v e rd e n tu re
prosthesis m akes it possible to exten d th e d e n tu re base and rely on palatal and p osterio r d e n tu re
bearing areas fo r tissue s u p p o rt, in situations w ith 4 im plants o r fe w e r. W h e n p la c e m e n t o f a
sufficient n u m b e r o f im plants is feasible, th e s u perstru ctu re can be purely im p la n t s u pp o rted . In
such a situation o n e m ust m ake a choice b e tw e e n a fixed and re m o v a b le design. An a d vantage o f
m axillary o v e rd e n tu re s co m p ared to fixed p ro s th e s e s , is th a t im plan ts can o fte n be placed in th e
a n te rio r seg m en t o f th e m axilla b e tw e e n th e first p rem o lars, avoiding in te rfe re n c e w ith th e
sinuses. Congruence o f th e position o f im plants and pro sth etic te e th is not necessary, fa cilitating
m a n a g e m e n t o f ae s th e tic concerns, such as to o th position, soft tissue c o ntou r, and facial
m orphology and su pp o rt. A dvantages o f fixed o r re m o v a b le prostheses have been listed in
decreasing o rd e r as th e y re la te to th e m a x illa /m a n d ib le as su m m arized by Strassburger (figure
13) [27]. He proposes this ta b le be used to in fo rm p atien ts b e fo re a tr e a tm e n t decision is m ad e ,
as it shows th e d iffe re n t advantages o f both types o f prostheses, depen d in g on w h e th e r th e y are
Maxilla
Mandible
Removable
Speech Function
Ease of Cleaning
Ease of Cleaning
Aesthetics
Aesthetics
Stability
Fixed
Comfort
Stability
Speech Function
Chewing Ability
Stability
Ease of Cleaning
Figure 13. Advantages of fixed or removable prostheses dependant on M x ./M n d (Strassburger 2006)
Prosthesis Survival/Success:
It is im portant to distinguish between implant prosthesis survival and success. Survival implies that
the restoration in question is simply still there and is a considerably lower burden to achieve than
success. Success is a set of standards usually set on a prosthesis type basis that sets out the
acceptable and desirable minimum requirements of a restoration from a technical, aesthetic or patient
stand-point .Thus, to be considered successful, an implant has to meet certain criteria in terms of
function, tissue physiology,absence of pain and other pathological processes , patient satisfaction
(aesthetics and absence of discomfort) and maintenance of osseointegration, [57].
A lack o f standardization o f prosthetic procedures, num ber o f im plants, marginal bone
measurements, bone quantity, and loading conditions, as w ell as insufficient sample size, have
hindered an objective assessment o f the success o f im plant overdentures and com plete fixed
[image:56.524.6.516.29.723.2]