Institutionen för vård och natur
Nursing documentation before and after implementation of
electronic patient records.
Omvårdnadsdokumentationen före och efter implementering av
elektronisk patientjournal.
Examensarbete i omvårdnad, D-nivå 10 poäng
Vårterminen 2007
Författare: Ulveborg, Helene
SAMMANFATTNING
Titel: Omvårdnadsdokumentationen före och efter implementering av elektronisk patientjournal.
Institution: Institutionen för vård och natur, Högskolan i Skövde Kurs: Examensarbete i omvårdnad D-nivå, 10 poäng Författare: Ulveborg, Helene
Handledare: Eriksson, Nomie; Bergh, Ingrid
Sidor: 25
Månad och år: Januari 2007
Nyckelord: Omvårdnadsdokumentation, implementation, elektroniska patientjournaler, kvalitet, granskning, enkät
Syfte: Att beskriva kvalitetsförbättringar och sjuksköterskors åsikter angående omvårdnadsdokumentationen, efter implementering av elektronisk patientjournal.
Bakgrund: Tidigare studier visar att dagens omvårdnadsdokumentation är bristfällig både gällande innehåll och struktur. Dessa förhållande hindrar vårdgivaren att få en snabb åtkomst till relevant patientinformation. Implementering av ett elektroniskt patientjournalsystem kan ge sjuksköterskorna ett effektivt verktyg för omvårdnadsdokumentation, men det förutsätter även att sjuksköterskan, förutom basal datorkunskap, har dokumentationskunskap i hur och vad som ska dokumenteras för att kunna öka dokumentationskvaliteten. I annat fall kommer hälso- och sjukvården enbart att datorisera de befintliga dokumentationsbrister som finns i
Metod: En retrospektiv journalgranskning av omvårdnadsjournalen gjordes med Cat-ch-ing instrumentet före och efter implementering av elektronisk patientjournal (n=25/25) för att undersöka om fastställda mallar med fördefinierade sökord ökar kvaliteten i elektroniska patientjournaler i jämförelse med tidigare pappersjournaler. Undersökningen kompletterades även med en 24-frågors enkät med en fyrgradig svarsskala, för att kunna reflektera sjuksköterskornas åsikter angående implementeringen av elektronisk patientjournal. Totalt 51 sjuksköterskor medverkade genom att besvara enkäten, svarsfrekvens 98%.
Resultat: Deskriptiv statistik samt Mann-Whitney-test användes för att analysera studiens resultat. Journalgranskningen visar att kvaliteten ökar med elektronisk patientjournal. Det är en signifikant skillnad i jämförelse med tidigare pappersjournaler, p < 0.001. Enligt mätinstrumentet Cat-ch-ing ökade den totala poängen med 53% till förmån för elektroniska patientjournaler. Enkätresultatet visar att de flesta sjuksköterskorna anser att den elektroniska patientjournalen och dess fördefinierade mallar underlättar deras arbete, trots att den inte upplevs tidsbesparande.
Konklusion: För att uppnå användar-tillfredställelse och ökad kvalitet i omvårdnadsdokumentationen, då man inför ett nytt dokumentationsverktyg, är det sannolikt av relevans att sjuksköterskorna själva ges möjlighet att påverka och planlägga sina egna förutsättningar för dokumentationen. Därför förefaller det betydelsefullt att sjuksköterskorna är involverade i det förberedande arbetet under implementeringsprocessen.
Abstract
Aim. To describe quality improvements and nurses opinions of nursing documentation after implementation of electronic patients records.
Background. Former studies states that today’s nursing documentation is insufficient both concerning journal content and poor structure. These circumstances prevent caregivers to prompt accessibility to relevant patient information. Implementation of electronic patient records systems could give nurses an effective tool for nursing documentation, but it also demands that nurses, except of basic computer knowledge, have knowledge in how and what to document in order to increase quality in documentation. Otherwise health care organisations just computerise existing insufficient in paper journals.
Methods. A retrospective audit of nursing records with Cat-ch-ing instrument was performed before and after implementation of electronic patient records (n=25/25) to investigate if stipulated templates with predefined keywords in electronic patient records increase quality in nursing documentation on comparison to former paper journals. Also a 24-item questionnaire graduated in four levels was accomplished at the same hospital ward to reflect nurses’ opinion of implementation of electronic patient records. Totally 51 nurses participated by answering the questionnaire, response rate 98%.
Result. Descriptive statistics and Mann-Whitney-test were used to analyse study result. Audit of records shows that quality in documentation increase with electronic patient records. There is a significant difference in comparison to former paper journals, p < 0.001. With Cat-ch-ing measure instrument total score increased with 53% in favour to electronic patient records. According result of questionnaire most nurses consider that electronic patient records and its stipulated templates facilitate their work, though it is not consider timesaving.
Conclusion. To achieve user-satisfaction and increase quality in nursing documentation it is presumably important that nurses as professionals is given opportunity to influence and design their own prerequisites for documentation, when implementing a new documentation tool. Therefore it seems significant that nurses are involved in this preparatory work during implementation process.
Keywords: Nursing documentation, implementation, electronic patient records, quality, audit, questionnaire
Table of contents
Introduction ... 1
Quality aspects in nursing documentation... 2
Literature review... 5 The study ... 7 Methods... 8 Training program... 9 Data collection... 9 Instruments... 9 Nursing records... 11 Reliability/Validity... 12 Ethical consideration ... 12 Data analysis ... 13 Results ... 14
Audit of nursing records... 14
Questionnaire ... 15 Discussion ... 17 Limitations... 19 Conclusion... 20 Acknowledgement... 21 References ... 22
Tables:
Table 1. Description of nurses participation in different parts of training programs before implementation of EPR.
Table 2. Descriptive statistics of nurses that has answer the questionnaire. Table 3. Results from auditing nursing records with Cat-ch-ing instrument.
Table 4. Nurses opinion of education/knowledge, quality aspects and changes in nursing documentation after implementation of EPR.
Figures:
Figure 1. Aspects of quality and quantity in paper journals and EPR. Figure 2. Nurses satisfaction with education on comparison to age.
Appendices:
Appendix 1. Cat-ch-ing instrument (in Swedish). Appendix 2. Key to Cat-ch-ing (in Swedish).
Appendix 3. Authorization for investigator to acquaint information in patient records (in Swedish).
Introduction
Although Swedish nurses have been obliged to keep records since 1986, when the Swedish Patient Act (SFS 1985) was introduced, several studies shows there are considerable deficiencies in nursing records. These earlier findings indicate that qualities in today’s nursing documentation have not improved to higher extent than to fulfil function as a logbook (Ehrenberg et al. 2001, Törnvall 2004). This circumstance is also confirmed by an extensive Swedish research, in which Grufman Reje (2002) declare that a large number of journals have a common feature of poor structure, which prevents caregivers to get accessibility to relevant patient information and makes it hard to ensure continuity of care during patients trajectory through the health care system.
Just to implement an electronic patient record (EPR) neither solves the problems regarding insufficient quality in nursing records or well-arranged documentation, if nurses do not change their manner in what way they document patient care. The change to EPR emphasise the importance of documenting information that describes the actual caring process. But even if implementation of EPR give nurses a documentation tool that is effective in itself, it also demands that nurses have the skill to document in a more structured way (Moen et al. 1997, Newton 1995). If the public sector do not wish to computerize existing deficiency in nursing documentation when introducing a computer based journal system in a hospital, there is a need of united effort to define prerequisites so quality in nursing record at least fulfil demands described in laws and directives (Grufman Reje 2002). In order to achieve an increased quality and to create opportunities for a good structure in documentation there is, according to earlier studies, a conclusive condition that nurses have opportunity to influence the
performance of nursing documentation system before implementing EPR (Larrabee et al. 2001, Moen 2003, Törnvall 2004).
Implementing EPR in a large organisation is expensive, consequently it is of great importance to estimate what benefits this will achieve. The purpose of this study is to investigate if use of computer-assisted documentation has provided increased quality in nursing documentation; therefore nursing records were audit retrospective with a validated measuring instrument (Cat-ch-ing) before and after implementation of EPR. The audit is also complemented with a questionnaire to examine nurses’ opinions of implementation of EPR concerning education/knowledge, time-aspects, if application is user-friendly and nurses interpretations of quality aspects in nursing documentation in comparison to former paper journal.
Quality aspects in nursing documentation
Measuring quality is to judge if quality is good or less good. Quality as conception concerns to which extent activities that are carried-out in public service correspond to established criteria and standards for what is consider to be a good and secure patient care (Donabedian 1988). Quality assurance in a specific domain is understood to continuous provide a detailed exploration for a separate activity, so one could follow up quality aspects eligible for this specific domain. It also means to attend and improve details for things that are not working or serve as they are supposed to do. Audit of records imply that knowledge in documentation is collected in a quality check-up so methods and processes that endorse quality is guaranteed (Ehnfors 2001). To manifest quality in nursing documentation knowledge is required about different methods for developing and measure quality. Quality in nursing records can not be precise by an absolute score that speaks for itself as a whole, but by divide quality conception in different elements, there are a number of quantitative variables that could be objectively
measured (Idvall et al. 1997). A quality indicator in nursing documentation could be defined as a quantitative measure, in which variables about structure, process and outcome could be used as guidance and criterion to promote quality improvement in nursing records. Cat-ch-ing instrument conform to criterion of nursing documentation that rely on a quality indicator established by The Swedish Society of Nursing (Ehnfors 2001).
Nursing documentation implies something more than just record separate facts and observations about patient care. Documentation should reflect patient’s own individualized experience of health situation. Nursing documentation should also be based upon the scientific nursing knowledge which is fundamental for the nursing profession. In contrary to this announcement Heartfield (1996) express: “Difficulty in documenting occurs because nurses generally deal intimately with events people do not want to know about” (p. 99). This could be one of the main reasons that nursing documentation to a large extent has a medical technical approach to patient problems, a perspective where nurses appears as invisible assistants. These facts are not favoured by that holistic perspective that ought to characterize nursing as a profession (Brooks 1998, Heartfield 1996). An argument supported by Benner (1993), who means that specific nursing knowledge would not be perceptible before nurses can verbalize and document their experiences. Nilsson and Willman (2000) states: “Documentation that is well performed is of crucial importance for both the quality of nursing care and the development of nursing knowledge, as well as being one of the prerequisites of quality assurance within nursing” (p. 199).
In allusion to make nursing documentation available to others, nurses should communicate in a more distinct and professional way, in other words making nursing actions more explicit and expressed in a more effective way. One way to achieve this purpose is to design nursing
records in accordance to nursing process (Ehnfors et al. 1993). When Yura and Walsh (1987) describe nursing process in four separate steps this transformed emphasis from a former intuitive approach to a more nursing expertise orientation. Nursing process is a theoretical model for problem-solving. This model illustrates nursing practice as a conscious reflection made by nurses concerning assessing, planning, implementing and evaluation of patient-care (Ehrenberg et al. 2001). Just like physicians prescribe medical care plans to treat patients diseases adequate and with medical liability, nurses use nursing process to establish care plans so patients nursing problems is treated in an adequate and responsible way (SOSFS 1993a, 1993b). A study by Newton (1995) shows that use of nursing process in documentation increases nurses’ awareness of patients need for care and this will also improve nurses’ ability to identify essential nursing actions; it will also facilitate further nursing research and practice.
Several studies points out certain aspect that should be documented in nursing record in accordance to receive a credibility- and professional perspective. Those studies indicate that journal content should be precise, documented with actual accuracy to highest possible extent, even due lack of time, because of its importance as information source for clinical evidence reports. Documentation is the main source to information and evidence used for dealing with incidents, claims or complaints from patients, relatives or Medical Responsibility Board (Mahler 2001, Pennels 2001, Wood 2003). Pennels (2001) specify that in all clinical journals there is an obligatory documenting: identification over who written the notes – and in cases of digression all staff involved in accidents or disputes, legibility of documentation, notes must be dated and timed in chronology order and journal documentation should avoid abbreviations – documentation must be comprehensible even if person is not familiar to wards particular speciality. Journal content should not contain any unprofessional or disparaging remarks –
journal could be referred to and read by many different sources, for example patient, relatives, Medical Responsibility Board or law court if incident or claim is being investigated. All aspects depict in Mahler, Pennels and Woods rapports, is also found in Swedish laws and directives regarding nursing documentation (SFS 1985, SOSFS 1993a, 1993b).
In Sweden VIPS is an applied model for nursing documentation, with keywords developed in accordance with nursing process. VIPS is an acronym for the Swedish words Välbefinnande (Wellbeing), Integritet (Integrity), Prevention (Prevention) and Säkerhet (Security), conceptions that should characterize good patient care (Ehnfors et al. 1991). This documentation model was applied in Sweden 1991, and outlines the guiding principles to documentation according to nursing process and proposes keyword that nurses could use to facilitate journal content (Nilsson & Willman 2000). VIPS-model is also applied in neighbouring Nordic countries and has been tested and validated in several different studies (e.g. Ehrenberg et al. 1996). Ehnfors and Smedby (1993) consider that if nurses are given opportunity and equipment that is necessary to document according to nursing process and VIPS-model, this would be a guarantee that intentions in Swedish Patient Act are to be fulfilled.
Literature review
Nursing documentation has not attained that impact that was supposed. A reason for this could be that nurses has a verbally tradition to relay on in their communication to other caregivers (Brooks 1998, Ehnfors & Smedby 1993, Heartfield 1996). Documenting nursing actions was a new innovation when Swedish Patient Act was introduced. Former documentation had commonly manifested activities prescribed by physicians (Ehnfors & Smedby 1993). On wards changing from oral shift reports to reading written records nurses
have complain about an imperative necessity in reading a large quantity of notes in order to get the hang of patients situation, this is consider very time-consuming. One reason for this is that many notes are documented more than once in a journal (Björvell et al. 2003). Different nurses has documented same problem over and over again, because of poor structure they can not find what already has been notified about patients problem. Lack of time, an undisturbed working environment or nurses not being familiar with documenting in accordance with the nursing process are some of the most common elements that nurses report as reason to poor, inadequate documentation (Björvell et al. 2003, Brooks 1998, Kim & Park 2005).
There are only a few studies that valuate what impact EPR have on quality aspects in nursing documentation. None of these earlier studies is possible to apply to hospital care in Swedish health care organisation. Two separated studies (Larrabee et al 2001 and Smith et al. 2005), shows ambiguousness results whether computerization will improve quality aspects in nursing documentation or not. In contribution Nahm (2000) state that computer-assisted documentation will increase the quality in documentation. In her article she also criticizes earlier studies that have valued quality aspects after implementing EPR. She means that these studies were not made by equal data collections or in same hospital wards, some of these studies does not even compare the same hospitals. Nahm means that under these circumstances one could not compare quality aspects at all. Hellesø (2006) compared quality in nursing discharge notes before and after computerization and found that journal quality increased both in structure and substantial contents. She means that predefined keywords in EPR will facilitate for the nurse to focus on adequate nursing content in documentation.
Consequently, the investigator observed that several studies were carried out in purpose to valuate quality aspects in nursing documentation. Only a few studies has valuated if impact of computer-assisted documentation could bring increased quality in nursing documentation, facts that motivated this study.
The study
The aim of this study is to examine if implementation of EPR has increased quality in nursing documentation.
• Does an audit of nursing records show any differences in quality after implementation of EPR in comparison to former paper journal?
• What are nurses’ opinions of EPR implementation regarding performance of nursing documentation application, documentation structure and influences on their way of working?
• Are nurses user-perspective of EPR reflected in result from audit of quality aspects in nursing records?
Methods
This study is carried-out in a cardiac ward at a middle-sized hospital in west Sweden. In earlier quality check-up’s made by investigator before implementation of EPR, quality in nursing documentation has been equivalent between wards at hospital. Investigator is familiar with most specialities in the hospital; therefore decision of auditing nursing records at the cardiac ward was just a coincidence.
As pointed out in earlier studies it is important that nurses receive opportunity to influence implementation process of EPR in order to achieve increased quality and to create opportunities for a good documentation structure in nursing records (Larrabee et al. 2001, Moen 2003, Törnvall 2004). The investigator and a nurse colleague therefore participated during whole implementation process when EPR (Siemens Melior 1.5) were implemented at this hospital. Investigators part in this implementation process was to develop an effective documentation structure in EPR-application and prepare stipulated templates that are user-friendly. The investigator was also commissioned to develop clear policies and guidelines for nursing documentation at the hospital.
To respond to the aim of this study and to answer research questions two different methods were applied, audit of nursing records and a questionnaire. Study intervention in reviewing nursing records consists of an analyse to investigate if stipulated templates with predefined keywords in EPR increase quality in nursing documentation on comparison to former paper journals, in which the nurse him/herself structured his/her nursing notes and selected relevant keywords. The investigator also wanted to estimate how nurses have interpreted implementation of EPR and what nurses consider of quality aspects in documentation after this implementation, which motivated the questionnaire.
Training program
During implementation process nurses were offered education in basic computer knowledge and word processing. Nurses had to estimate themselves how much training they needed; none, half a day or one day. In this case 51% did not think they needed any education at all (see Table 1). Nurses also could select period of training time in EPR-application, one day or half a day, this education was compulsory. Most nurses, 80% had one day of education. All nurses were educated in nursing process and nursing documentation during a 2 hours lecture. Nurses that needed personal supervision in documentation or EPR-application were offered this during first week of implementation. Training program during implementation process was equivalent to all wards at the hospital.
INSERT TABLE 1 ABOUT HERE
Data collection
Instruments
Data collection in this retrospective audit is built on an indirect observation based on a measure instrument called Cat-ch-ing. Björvell, Thorell-Ekstrand and Wredling (2000) developed this instrument. Cat-ch-ing instrument claims to measure formal structure, quality and quantity in nursing documentation. Result from former studies made to compare reliabilities coefficient between different measurement tools for auditing journals, shows that if the instrument have a correlation is about 0,70 (Pearson’s correlation coefficient) is consider as reliable. In comparison to other measuring instruments Cat-ch-ing received a high reliability coefficient on 0,98 (ibid).
Measure instrument Cat-ch-ing observes structure according to the nursing process and also judge journal content. This instrument consist of totally 26 items (score 0-3) divided in two parts; one quantitative judgement and a qualitative judgement (see Appendix 1). This two parts could together reach a score at maximum 80 points per journal (passed with distinction) if all variables could be identified, if it is signed and dated correctly. In manual “Key to Cat-ch-ing” authors has specified what criterions in journal content that has to be fulfilled to receive a specific score in judgement (Appendix 2). Low score gives information about essential parts in nursing process are left out, while a high score could imply that the documentation is very good – but it could also means there is lack of substantial information because quality judgement is done entirely by notes that are documented in the nursing record (Björvell et al. 2000).
Earlier studies indicate there is a discrepancy between what actually has been done in patient care and what is documented (Brooks 1998, Hale et al. 1997). This is also confirmed in a study by Adamsen and Tewes (2000) in which result shows that only 31% of patients problem was documented in nursing records. These facts emphasize that an audit do not measure quality in caring that is performed, just quality in what has been documented.
To estimate if nurses consider implementation of EPR has increased quality aspects in documentation audit of records was complemented with a questionnaire in which 24 statements was developed. These statements are built on a four grades Likert scales and had answering parameters scored as an ordinal scale: Agree totally (1p), mainly (2p), partly (3p) or disagree (4p). Questionnaire was tested in a pilot study at another hospital ward in order to valuate if any adjustments of inquiries had to be done. Inquires require no changes. During September 2006 questionnaire was distributed by head nurse to all nurses working on the
ward. In introduction letter, which was accompanying together with a prepaid letter, was inferred that reply was required in 2 weeks. After this two reminders to reply questionnaire, at intervals of one week, were sent to head nurse, who was asked to remind nurses at ward to fill in and send back questionnaire. Respondents were guaranteed total anonymity. Totally 52 nurses, 10 male and 42 female are employed at this ward. Participation to study was voluntary. 51 nurses consent to participate by answering the questionnaire (n=51), total response rate 98%. For descriptive statistics see Table 2.
INSERT TABLE 2 ABOUT HERE
Nursing records
Patient records were collected before the hospital started implementation process and then 8 months after implementing EPR. To what extent computerization have influence on documentation could not be evaluated until 6 months after implementation, according to a study by Larrabee et al (2001). Selected records were randomised in a methodical procedure. Criterion was all patients discharged on Mondays in September 2003 and May 2006. Patients are discharged from ward all days of the week, Mondays is just a coincidence. All patients that were discharged on Mondays were included independently of their diagnosis or length of stay. Of this reason investigator could not predetermined number of records to audit, but randomisation gave an equivalent numbers of journals, 25 before and 25 after implementation of EPR (n=25/25). To find out identity of these patients, information was collected from hospitals´ administrative system.
Reliability/Validity
Reliability in audit of this study is based on a retrospective review of nursing records; the performance of documenting could therefore not been modified by nurses afterwards. Audit of records could be compared on equality with data from a qualitative content analysis. There is always risk of a subjective interpretation. To achieve reliability in study result of audit investigator should not interpret things into journal content that is not written-down (Graneheim & Lundman 2004).
6
To assure validity in quality judgement, acute or contemplated admissions should be directly to hospital ward, in which this study is carried-out. This has excluded patients that were shifted between different hospital wards, because nursing documentation then had been made by other nurses on other wards. When shifting patients between hospital wards it is common to just document a résumé of nursing actions in a nursing note. In other words there is no discharge note made, criterion that had excluded patient because presence of discharge note is a variable for judgement according to Cat-ch-ing instrument. Five paper journals and four EPR did not fulfilled to study criterion and were consequently declined.
Ethical consideration
Review took place in hospital locality. Audit was made in original case report; therefore no paper copies were made. To take part of information in a patient record a person should have a relationship to patients as being part of nursing staff, circumstances that investigator did not fulfil. By request from Ethical committee hospitals Chief of Medical Division authorised investigator to acquaint information in patient records (Appendix 3). No patient identity information will be revealed by investigator according to professional secrecy. The Personal Data Representative at the hospital approved use of patient data from hospitals administrative system.
Data analysis
Auditing journals means to systematic analyse journal content. A structured examination protocol gives judgement to each separate journal. To achieve an overall impression of documentations the investigator read all written documentation from hospital care episode, independent of what profession that had documented this notes. After this survey a new review were made focussing on exclusively nursing documentation. In this study the investigator has systematically auditing variables according to manual “Key to Cat-ch-ing” (Appendix 2) (Björvell et al. 2000).
In questionnaire respondents could chose one of four given alternatives to reply to statement; agreement in three different levels (totally, mainly or partly) or respondents could disagree to statement. The four respond alternatives were analysed separately.
To calculate variables in Cat-ch-ing instrument and from questionnaire, statistical data analysis processing was performed was performed in Excel 97 and SPSS 11.5. Data collection is mainly analysed by descriptive statistics; percentage, mean, range and standard deviation (SD). Mann-Whitney-test was used as nonparametric test to compare differences between independent samples in audit. Hellesø (2006) made a power calculation, in which she computes that 16 records from each group is a minimum to calculate differences between paper journals and EPR, and to estimate significance 0.05. To test significance in this study investigator could use 25 records from each group to estimate p-value < 0.05.
Results
Audit of nursing records
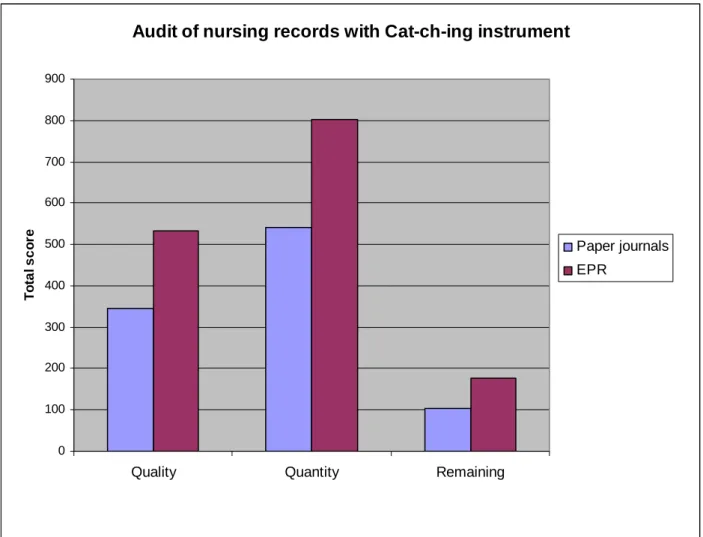
Each record could reach a maximum score at 80 points per journal. 25 records could therefore receive a total score of 2000 points. In result of audit with Cat-ch-ing instrument the total score increased with 53% in advantage to EPR (total score 1513, n=25) in comparison to former paper journal (total score 987, n=25). There was a significance difference between groups, p-value < 0.001. Before computer-based documentation score range per journal 18-55 (mean 39.48) and with electronic documentation score range 41-79 (mean 60.52). Almost every variable in Cat-ch-ing instrument received a higher score in EPR with exception for variable about quantity for planned interventions that was lower than former paper journal (see Table 3). The highest enlargement was received by variable Nursing status at discharge, both quality and quantity aspects had increased with 100% each, because of total absence of this in paper journals. A discharge note was found in every nursing record in EPR, in audit of paper journals there was only one record with a discharge note. In one paper journal all information about year-dating where missed. In EPR-application this is automatically updated by programme when a new note is made. According to manual “Key to Cat-ch-ing” referring to variable ´Is the record legible´ records could only reach score of 3 if it is typewritten which is favourable to EPR-application, but all notes in paper journal was legible and therefore all received score of 2.
Both quality and quantity aspects increased with EPR. Also remaining variables in Cat-ch-ing concerning if primary nurse is indicated and variable about if there is a discharge note increased with EPR (Figure 1).
INSERT FIGURE 1 ABOUT HERE
Though quantitative column increased with EPR as shown in bar chart in Figure 1, this fact does not signify that nursing notes were increased in numbers in EPR. On the contrary there was a reduction of nursing notes in EPR. Instead notes were more quantitative complete according to judgement in manual “Key to Cat-ch-ing which gave a higher total score. Former running notes that was applied in paper journal was instead collected and structured in stipulated templates for nursing status and in care plans in EPR, which decreased number of separate running notes. In paper journal there was a great amount of nursing notes concerning what physicians had prescribed on daily medical rounds among patients. During implementation process this workflow was changed. In EPR physicians had take over this function and make their own notes for a daily basis of what they themselves has prescribe. This could also be one of the main reasons for reduced number of notes in nursing records.
Questionnaire
The questionnaire consisted of 24 statements sorted in four subheadings; Education/knowledge, Time, User-friendly application and Quality aspects in nursing documentation. Nurses answered statements with one of following alternatives; totally agree, mainly agree, partly agree or disagree. Statements were scored 1 to 4, low score is consider positive, see table 4.
INSERT TABLE 4 ABOUT HERE
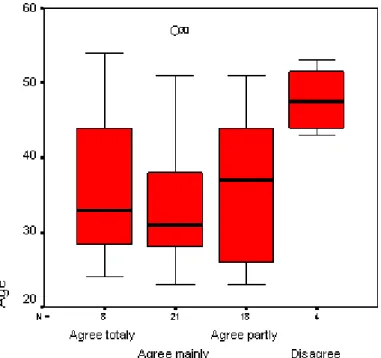
According to questionnaire result main part of nurses thinks that EPR facilitate theirs work and gives better accessibility to patient information. They often read other professionals documentation. But in the same time 16% of nurses did not think EPR makes it easier to find information about patients’ problems. Only 2% of nurses think they have enough time to document and the main part did not think they have an undisturbed working environment. All nurses agreed that stipulated templates in EPR facilitated their selection of keywords, but there was a divergence in knowledge skill of how and what to document. 4% of nurses’ did not feel familiar to documentation accordant to nursing process while 8% of respondents did not think they have enough knowledge about laws and directives concerning documentation. Nurses at ward are aware that they commonly use abbreviations specific to ward, this was also seen in audit of records. Most nurses were quite satisfied with education and training program they received during implementation process. But there was a certain deviating in proportion to age. Older nurses seemed less satisfied, see Figure 2. Gender was of little consequence to grade of satisfaction.
Discussion
Without doubt quality and structure has increased in nursing documentation after implementation of EPR according to audit result. These facts are also reflected by nurses’ opinions about EPR. Nurses consider EPR to be a tool that facilitates their work. Stipulated templates with predefined keywords facilitate for nurses to document, though EPR-application is not consider timesaving. Respondents in common had a positive attitude to EPR. But lack of time and undisturbed environment is still factors that nurses estimates as insufficiencies in documentation irrespective of documentation-media. This result from questionnaire conforms to earlier study result by Björvell et al (2003), Brooks (1998) and Kim & Park (2005).
In order to improve patient security nurses have a professional responsibility to ensure the safety, continuity and quality of patients’ care by accurately recording relevant information (e.g Mahler 2001). In this study audit of records revealed that nurses sometimes had noted relevant information of patient problem in status on arrival, but after this investigator could not found any note or evaluation of this. Have nurses followed up patient problems but not documented this? This sort of problem is comparable to what Hale (1997) and Adamsen & Tewes (2000) found in their research. There was also meagre documented what information patient received about health situation and actions, both planned and implemented and what follow-up there would be after patients discharge. Earlier studies point out that discharge notes often is missing in nursing records (Grufman Reje 2002, Hellesø 2006). These facts were also seen in audit of paper journals in this study. But after implementation of EPR there was found a discharge note in every record, reports that stand in opposition to what other research had found. One reason for this could be that most nurses at ward, according to result
in questionnaire, have good knowledge about guidelines and policies for documentation that was pointed out before implementation of EPR.
Though most nurses seems to think that documentation is focussing on what nurses performs, there still is a big influence of medical technical approach in nursing documentation, and this has not change in the new media. Investigators subjective conclusion of audit concerning content in nursing records is that nurses remain invisible medical assistants as shown in earlier studies (Heartfield 1996, Törnvall et al. 2004). A positive effect in nursing documentation was that double-documentation between different nurses has almost disappeared in EPR comparatively to paper journal. But there is still information double-documented between different professionals in patient records. Above all this is obvious on patients’ arrival there physiological measurements are duplicated between nurses and physicians. Have physicians themselves made this measurement? To investigator these measurements seemed to be a genuine copy of what nurses already had documented in patient record. In other parts of EPR double-documentation were quite rare between different professionals. To form a complete picture of patients situation in audit investigator could only achieve this when reading all professionals notes. These facts correspond to what respondents have answered to statement ´I often read patient information documented by other professionals. This must be considering as a positive development in EPR in comparison to former paper journal. In guidelines and policies for documentation that was established before implementation of EPR, it was mentioned that double-documentation between different professional presumably do not benefit patients care. Therefore guidelines and policies for documentation recommended personnel to work as a multidisciplinary team and use each other’s documentation to achieve best possible care of patient and to minimise double-documentation, facts that seems to been responded by nurses according to study result in
nurses were more focussed on documenting their own nursing actions and nursing perspectives in patient care.
Limitations
Nursing process is accepted as a model in nursing documentation, though it has been questioned in earlier studies (Moen et al. 1997). Cat-ch-ing instrument measure how well documentation is performed according to the nursing process. But Cat-ch-ing instrument in itself do not take in account how well documentation is performed according to existing laws and directives, which is to be considering as an insufficiency with Cat-ch-ing instrument. How many score is required for a journal to obtain a pass? In manual to Cat-ch-ing no amount is given to what is consider bad or good – only passed with distinction, which is a limitation with this instrument.
Nahm (2000) stated the importance of equal data collection and to carry out studies at the same wards and with the same measuring instrument on comparison of documentation quality. But even if present study has been carried-out with equal data collection on the same ward – could one declare that there is implementation of an EPR-application in itself that has produced a positive study result? Earlier studies indicate that education interventions increases quality in nursing documentation (e.g Björvell et al. 2003); has a two hours lecture in nursing documentation promoted a part of the result? Or have guidelines and documentation policies that were established during implementation contributed to result? This ward has also had enthusiasts that have been prime movers to nursing documentation during implementation process. Does implementation of EPR in itself makes a mountain out of a molehill? To accumulate evidence for testing if EPR-application in itself brings increased quality effects in documentation investigator should perform an identical replication study
with exact duplication in methods and sampling criterions on another hospital ward but without any lecture or access to documentation guidelines. Universal applicability in this study could be consider limited because it is carried-out in one single hospital ward and has a small sample of 25 records. In result of questionnaire investigator choose to separately analyse the four answering levels in questionnaire, a choice that also could influence and make discrepancy to the positive overall impression in result, above all distinction between answering parameters Partly agree and Disagree.
As former studies pointed out it seems important that nurses are involved in preparatory work during implementation process of EPR, in order to influence and design nurses own prerequisites for documentation and to achieve user-satisfaction (Larrabee et al. 2001, Moen 2003, Törnvall 2004). In this study nurses was involved in this preparatory work by preparing stipulated templates with predefined keywords and also establish guidelines and policies to documentation. But to what extent this preparatory work has promoted part in result can not been verified in this study.
Conclusion
Result in this study shows that implementation of EPR-application is a good investment for health care organisation both concerning quality aspects in documentation and to user-satisfaction. This study affirms that implementation of EPR increase quality in nursing documentation. But there still remain a few aspects to increase documentation quality in further direction. Documentation skill has to be developed additionally so nurses feel confident in how and what to document and nurses also have to focus more on nursing experiences in documentation of patient care in order to achieve a substantial and holistic perspective in nursing profession.
Acknowledgement
References
Adamsen L., Tewes M. (2000). Discrepancy between patient’s perspective, staff’s documentation and reflections on basic nursing care. Scandinavian Journal of Caring Science 14: 120-29
Benner P. (1993). From Novice to Expert. Excellence and Power in Clinical Nursing Practice. Swedish Edition. Studentlitteratur, Lund
Björvell C., Thorell-Ekstrand I., Wredling R. (2000). Development of an audit instrument for nursing care plans in the patient record. Quality of Health Care 9: 6-13
Björvell C., Wredling R., Thorell-Ekstrand I. (2003). Improving documentation using a nursing model. Journal of Advanced Nursing 43 (4): 402-10
Brooks J. (1998). An analysis of nursing documentation as a reflection of actual nurse work. Medsurg Nursing 7 (4): 189-198
Donabedian A. (1988). The Quality of Care. How can it be assessed? JAMA 260 (12): 1743-8
Ehnfors M. (2001). Kvalitetsindikatorer inom omvårdnad. (Quality indicators in nursing). 3th edition. Förlagshuset Gothia AB, Växsjö (In Swedish)
Ehnfors M., Ehrenberg A., Thorell-Ekstrand I. (1991). Towards basic nursing in patients records. Vård i Norden 21: 12-31
Ehrenberg A., Ehnfors M., Thorell-Ekstrand I. (1996). Nursing documentation in patient records: experience of the use of the VIPS model. Journal of Advanced Nursing 24: 853-67
Ehnfors M., Smedby B. (1993). Nursing Care as Documented in Patient Records. Scandinavian Journal of Caring Science 7:209-20
Graneheim U., Lundman B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nursing Education Today 24: 105-12
Grufman Reje. (2002). Management. Ändamålsenlig vårddokumentation i Skåne och Västra Götaland. (Expedient journal documentation in Skåne and Västra Götaland) Commission report. Stockholm (In Swedish)
Idvall E., Rooke L., Hamrin E. (1997). Quality indicators in clinical nursing: a review of the literature. Journal of Advanced Nursing 25: 6-17
Hale CA., Thomas LH., Bond S., Todd C. (1997). The nursing record as research tool to identify nursing interventions. Journal of Clinical Nursing 6: 207-14
Heartfield M. (1996). Nursing documentation and nursing practice: a discourse analysis. Journal of Advanced Nursing 24: 98-103
Hellesø R. (2006). Information handling in the nursing discharge note. Journal of Clinical Nursing 15: 11-21
Kim YJ., Park HA. (2005). Analysis of nursing records of cardiac-surgery patients based on the nursing process and focusing on nursing outcomes. International Journal of Medical Informatics 74: 952-59
Larrabee J., Boldreghini S., Elder-Sorrells K., Turner Z., Wender R., Hart J. (2001). Evaluation of documentation before and after implementation of a nursing information system in acute care hospital. Computer in Nursing 19 (2): 56-65
Mahler C. (2001). Just the facts, please. A guide to effective documentation. Home Care Provider August:120-5.
Moen A. (2003). A nursing perspective to design and implementation of electronic patient record systems. Journal of Biomedical Informatics 36: 375-8
Moen A., Hellensø R., Olsen M. (1997). Nursing documentation – beyond the question of structure. Vård i Norden 17: 26-9
Nahm R. (2000). Measurement of the effects of an integrated, Point-of-care computer system on quality of nursing documentation and patient satisfaction. Computers in Nursing 18 (5): 220-9
Newton C. (1995). A study of nurse’s attitudes and quality of documents in computer care planning. Nursing Standard 38 (9): 35-9
Nilsson UB., Willman A. (2000). Evaluation of nursing documentation. A comparative study using the instruments NoGa and Cat-ch-ing after an educational intervention. Scandinavian Journal of Caring Science 14 (3):199-206
Pennels C. (2001). The art of recording patient care information. Professional Nurse 16 (9):1359-61
SFS (1985). Svensk författningssamling. Patientjournallag 1985:562 (The Patient Record Act) (In Swedish).
Smith K., Smith V., Krugman M., Oman K. (2005). Evaluating the impact of computerized clinical documentation. Computers in Nursing 23 (3): 132-8
SOSFS (1993a). Socialstyrelsens föreskrifter och allmänna råd om patientjournallagen 1993:20 (Advisory intructions of the Patient Record Act) (In Swedish)
SOSFS (1993b). Socialstyrelsens allmänna råd om omvårdnad 1993:17 (Advisory instructions on nursing) (In Swedish)
Törnvall E., Wilhelmsson S., Wahren LK. (2004). Electronic nursing documentation in primary healthcare. Scandinavian Journal of Caring Science 18: 310-7
Wood C. (2003). The importance of good record-keeping for nurses. Nursing Times January 14-20; 99 (2):26-7
Yura H., Walsh MB. (1987). The nursing process: assessing, planning, implementing and evaluating. 3rd edition. New York: Appleton-Century-Croft
Table 1. Description of nurses participation in different parts of training programs before implementation of EPR (n=51).
Acquired education n (%) Male Female Age mean (range)
Basic computer knowledge
One day 17 (33) 2 15 39 (24-57)
Half a day 6 (12) 1 5 27 (23-37)
None 26 (51) 6 20 36 (23-54)
Missing 2 (4) 0 2 35 (25-44)
Education in EPR application
One day 41 (80) 7 34 38 (24-57)
Table 2. Descriptive statistics of nurses that has answer the questionnaire (n=51). Data Gender - Male 9 - Female 42 Age - Mean 36 - SD 10 - Range 23-57 Years of practice - Mean 8 - SD 9 - Range 0-35
Table 3. Results from auditing nursing records with Cat-ch-ing instrument. Judgement variables in Cat-ch-ing instrument
(scale 0-3)*
Quality: Very good = 3, Good = 2, Less good = 1, Poor = 0 Quantity: Complete = 3, Partly = 2, Occasional = 1, None = 0
Paper journals (mean) n =25 EPR (mean) n = 25 p-value
Is there a primary nurse indicated:
• No - score 0
• Only by surname - score 2 3.92 4.0 ns**
• By surname and Christian name - score 4
Is there a nursing history: - quality 2.52 2.88 0.022
- quantity 2.84 2.88 ns
Is there a nursing status:
• On arrival - quality 2.0 2.72 0.002 - quantity 2.0 2.6 0.001 • Updated - quality 1.72 2.0 ns - quantity 1.6 2.0 ns • At discharge - quality 0 1.96 <0.001 - quantity 0 2.04 <0.001
Is there a nursing care plan:
• Nursing diagnosis - quality 0.44 1.16 0.026
- quantity 0.4 1.32 0.012
• Expected outcome - quality 0.12 1.04 0.003
- quantity 0.12 1.08 0.002
• Interventions planned - quality 1.48 1.56 ns
- quantity 1.56 1.48 ns
• Interventions implemented - quantity 1.67 1.96 ns
Is the underlying information for the nursing
diagnosis described in nursing status - quantity 1.92 2.56 0.015
Is nursing outcome described - quality 1.32 2.32 0.002
- quantity 1.2 2.36 <0.001
Are the VIPS keywords used
(regarding history, status, interventions) - quality 2.16 2.68 0.014
- quantity 1.92 2.8 <0.001
Is there a nursing discharge note - score 0-4 0.16 3.12 <0.001 Are all entries dated (years, month, day) - quantity 2.44 3.0 <0.001
Are all entries signed - quantity 2.44 2.88 0.002
Is there a clarification of signature - quantity 1.6 3.0 <0.001
Is the record legible - quality 2.0 3.0 <0.001
* Excluded first variable about Primary nurse indicated and Nursing discharge note, score 0-4 ** ns: not significant
Table 4. Nurses opinion of education/knowledge, quality aspects and changes in nursing documentation after implementation of EPR (n=51).
Statements Mean ± SD Percentage
*1 2 3 4 Education/knowledge
1. I am satisfied with the education/training program I received
during implementation process of EPR. 2.35 ± 0.84 16 41 35 8
2. I have enough education/knowledge about how to document. 2.47 ± 0.67 4 51 39 6 3. I have enough education/knowledge about what to document. 2.14 ± 0.57 10 66 24 0 4. I consider myself to have enough knowledge about laws and
directives concerning documentation. 2.02 ± 0.73 16 41 35 8
Time
5. I have enough time to document what I should. 2.57 ± 0.73 2 51 35 12 6. I estimate that I use less time to document in EPR than former
paper journal. 2.85 ± 1.09 15 23 25 37
7. Documentation takes to much time from patient care. 2.43 ± 0.78 11 49 40 0
User-friendly application
8. EPR is a tool that facilitates my work. 1.96 ± 0.75 24 62 8 6
9. EPR gives better accessibility to patient information than
former paper journal. 1.92 ± 0.74 31 45 24 0
10. EPR makes it easier to find information about patient problems. 2.45 ± 0.9 12 47 25 16 11. Documentation structure in EPR is easy to understand. 2.18 ± 0.83 18 54 20 8 12. It is easy to know what template I should use. 2.45 ± 0.78 8 49 33 10
Quality aspects in nursing documentation
13. I feel familiar with documentation structure accordant to
nursing process. 2.27 ± 0.75 14 49 33 4
14. I am familiar with all keywords used in documentation. 2.12 ± 0.87 22 54 14 10 15. Stipulated templates facilitate my selection of keywords. 1.59 ± 0.49 41 59 0 0 16. I think that a care plan is an important component in nursing
documentation. 2.28 ± 0.78 14 50 30 6
17. I write care plans for each patient I am responsible for as a
primary nurse. 2.94 ± 0.92 8 22 39 31
18. Standard care plans increase quality in documentation. 2.08 ± 0.6 12 70 16 2 19. I have opportunity to document in an undisturbed working
environment. 3.33 ± 0.79 4 8 39 49
20. I could find the same information about the patient in many
different notes. 2.04 ± 0.78 28 40 32 0
21. I often read patient information documented by other
professionals. 1.6 ± 0.7 50 42 6 2
22. Documentation is always focussing on the work that my
profession performs. 2.0 ± 0.64 18 66 14 2
23. Abbreviations specific to wards speciality never occurs in EPR. 3.22 ± 0.79 0 22 34 44 24. I have good knowledge about hospital guidelines and policies
for documentation that was pointed out before implementation
of EPR. 2.04 ± 0.79 25 49 22 4
Score range from 1-4, low score is positive
Audit of nursing records with Cat-ch-ing instrument 0 100 200 300 400 500 600 700 800 900
Quality Quantity Remaining
To ta l s c o re Paper journals EPR
Figure 1. Aspects of quality and quantity in paper journals (n=25) and EPR (n=25). Remaining variables consider if nurses’ name is indicated and if there is a discharge note. All items; quality, quantity and remaining has a p-value < 0.001.
Figure 2. Nurses satisfaction with education on comparison to age.
Result of statement ´I am satisfied with the education/training program I received during implementation process of EPR´ (n=51).
Appendix 1.
GRANSKNINGSMALL ”CAT-CH-ING” © FÖR OMVÅRDNADSJOURNALER
Journalkod:__________________ Avd:____________ Sjukhus:______________ Datum:_________________ Granskare:_________________________________
1
= se nyckel till mallen Kvantitet1 Kvalitet2
siffror inom parentes anger poäng komplett – (3) mycket bra – (3) delvis – (2) bra – (2) OBS! Läs nyckeln noga. enstaka – (1) mindre bra – (1) inte alls – (0) torftig – (0)
Finns en ansvarig sjuksköterska nej (0) _____
angiven? endast med förnamn (2) _____
med för- och efternamn (4) _____
Finns omv anamnes? kvantitet:______ kvalitet:_____
Finns omv status: - vid ankomst kvantitet:______ kvalitet:_____ - uppdaterat under vårdtiden3 kvantitet:______ kvalitet:_____ - uppdaterat vid utskrivning kvantitet:______ kvalitet:_____ (ev. i epikrisen)
Finns vårdplan: - omvårdnadsdiagnos4 kvantitet:______ kvalitet:_____ - mål5 kvantitet:______ kvalitet:_____ - åtgärder: - planerade kvantitet:______ kvalitet:_____ - genomförda kvantitet:______
Är alla problem först beskrivna i
anamnes/status?6 kvantitet:______
Finns resultatet beskrivet?7 kvantitet:______ kvalitet:_____ Används VIPS sökord?8
(avser anamnes, status, åtgärder, rapportblad) kvantitet:______ kvalitet:_____ Finns en omvårdnadsepikris/slutanteckning? ja (4)______ nej (0)_____ (epikrisen granskas med Cat-ch-Ing Epi)
Är anteckningarna daterade (år, månad, dag)? kvantitet:______ Är anteckningarna signerade? kvantitet:______ Finns namnförtydligande till alla signaturer? kvantitet:______
Är texten läslig?9 kvalitet:_______
Appendix 2.
NYCKEL TILL GRANSKNINGSMALL ”CAT-CH-ING©”
Att granska omvårdnadsjournaler innebär alltid ett mått av subjektivitet. Det är därför inte meningsfullt att jämföra detalj-poäng mellan t ex olika sjukhus, kliniker eller avdelningar om det är olika personer som har gjort granskningen.
Referens vid användande av Cat-ch-Ing:
Björvell, C. Thorell-Ekstrand, I. Wredling, R. Developement of an audit instrument for nursing care plans in the patient record. Quality in Health Care 2000; 9: 6-13
1) GRADERING KVANTITET
komplett en fullständig anteckning med VIPS-sökorden
3 poäng anamnes:1 ”livsstil” används när det är relevant, i övrigt skall alla anamnes-sökorden vara med.
status:1 följande sju sökord skall vara med – kommunikation, kunskap, nutrition, elimination, aktivitet, sömn, psykosocialt – resten används när det är relevant avseende den enskilda patienten.
omvårdnadsdiagnos: någon form av problemformulering skall finnas för allt som föranlett en planerad åtgärd.
mål: skall finnas för varje angivet problem, antingen som ett separat mål per problem eller som ett mer övergripande mål som täcker alla problem. planerade åtgärder: skall vara formulerade – med sökord – för varje angivet problem och/eller statusanteckning som anger problem.
genomförda åtgärder: det skall tydligt framgå att de planerade åtgärderna är genomförda, akut insatta åtgärder som därmed inte är planerade i förväg, bedöms ej.
resultat: skall finnas beskrivet antingen som resultat eller som uppdaterat status, för varje problemområde som åtgärdats.
delvis minst 50% av ovan, dock ej komplett. Med eller utan sökord. 2 poäng
enstaka mindre än 50% av ovan, dock finns anteckning. Med eller utan sökord. 1 poäng
inte alls anteckning saknas. 0 poäng
1
Här anges en minimistandard för kirurg- och medicinavdelning. Varje vårdenhet eller specialitet kan själva avgöra vad som ska gälla som minimistandard avseende
användning av VIPS-sökord. Med minimistandard avses de funktionsområden (rubricerade med sökorden) som alltid ska vara beskrivna, resterande sökord skall självklart också användas, men endast då det anses relevanta för situationen.
2) GRADERING KVALITET (bedömning görs av de anteckningar som finns) mycket bra alla anteckningar är tydliga, språkligt korrekta, koncisa utan överflödig 3 poäng text och med, för bedömning, nödvändig information medtagen. bra > 50% av anteckningarna är som ovan, dock inte alla. En del 2 poäng innehåller eventuellt för mycket text, eventuellt saknas information,
språket är inkorrekt t ex fragmentariska meddelanden, ofullständiga meningar, egna förkortningar, möjlighet att misstolka finns.
mindre bra < 50% av anteckningarna är korrekta, dock finns korrekta anteckningar. 1 poäng
torftig över lag otydligt, språkligt inkorrekt, väsentlig information saknas. 0 poäng
3) UPPDATERAT STATUS
Innebär beskrivning av förändringar i patientens tillstånd över tid. När en förändring skett finns detta beskrivet under nytt datum och aktuellt sökord.
KVANTITET: Alla statusanteckningar som indikerat någon form av problem skall vara uppdaterade. Man skall tydligt kunna följa ”hur det har gått”.
4) OMVÅRDNADSDIAGNOS
KVALITET: 1 poäng ges om någon form av problem- eller riskidentifiering utan analys finns beskriven, 2 poäng ges om försök till analys finns med, om ej optimal, 3 poäng erhålles endast då en analys av problemet finns beskriven, t ex med ett relaterat till och leder till i ett korrekt sammanhang.
5) MÅLFORMULERING
KVALITET: 3 poäng erhålles då målet är formulerat som ett tillstånd hos patienten (ej en åtgärd för sjuksköterskan), är realistiskt, mätbart och tidsangivet.
6) PROBLEM BESKRIVNA I ANAMNES/STATUS
Här avses att bedöma huruvida de problem som finns angivna i vårdplanen, först finns beskrivna i anamnes/status. Om problemformuleringar saknas, finns det heller ingenting här att bedöma.
7) RESULTAT
Det är många gånger svårt att med säkerhet avgöra exakt vad resultatet är en effekt av, omvårdnadsåtgärder, medicinska åtgärder eller organismens egen ”läkningsförmåga”. Därför är det inte nödvändigt att resultaten är beskrivna i samband med åtgärderna, huvudsaken är att det i journalen går att hitta effekten hos patienten, t ex förändringar i dennes funktion. Det kan t ex vara beskrivet som ett uppdaterat omvårdnadsstatus. 8) ANVÄNDS VIPS-SÖKORD
KVALITET: bedöm om sökorden är korrekt använda, dvs rätt text under rätt sökord. Se VIPS-folder av Ehnfors, Thorell-Ekstrand, Ehrenberg.
9) LÄSLIG TEXT