Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Evaluation of the BD GeneOhm StaphSR Assay for Detection
of Methicillin-Resistant and Methicillin-Susceptible
Staphylococcus aureus
Isolates from Spiked
Positive Blood Culture Bottles
䌤
Sabine Gro
¨bner,
1Mireille Dion,
2Me
´lanie Plante,
2and Volkhard A. J. Kempf
3*
Institute of Medical Microbiology and Hygiene, University of Tu¨bingen, Tu¨bingen, Germany1; BD Diagnostics GeneOhm, Que´bec,
Canada2; and Institute of Medical Microbiology and Infection Control, University of Frankfurt am Main, Frankfurt am Main, Germany3
Received 13 November 2008/Returned for modification 30 January 2009/Accepted 3 April 2009
To improve the clinical outcome ofStaphylococcus aureussepticemia, the early selection of appropriate antibiotic treatment is crucial. Molecular diagnostics represents an attractive approach for the rapid identification of S. aureus and the determination of its methicillin (meticillin) resistance. In direct comparison to other molecular assays (sa442andmecAreal-time PCRs) and standard laboratory proce-dures, we evaluated the BD GeneOhm StaphSR assay for its use in the detection of S. aureus and methicillin-resistant S. aureus (MRSA) from spiked blood culture bottles (n ⴝ 134). In the case of detectingS. aureus (n ⴝ 90; for methicillin-susceptible S. aureus, n ⴝ 45; for MRSA, n ⴝ 45), the BD GeneOhm StaphSR assay had a sensitivity and a specificity of 100% each (95% confidence intervals [CIs], 96.0 to 100% and 82.4 to 100%, respectively). For MRSA (n ⴝ45), the test was 95.6% (95% CI, 84.9 to 99.5%) sensitive and 95.3% (95% CI, 86.9 to 99.0%) specific. Overall, five discrepant results arose with this assay due to the presence of methicillin-susceptible, revertant MRSA strains (3/45) and MRSA strains that were not detected by the BD GeneOhm StaphSR assay (2/45). Compared to other real-time PCR-based molecular approaches and to conventional standard laboratory methods, the BD GeneOhm StaphSR turned out to be an appropriate diagnostic tool for a rapid (⬃1.5 h), preliminary identification ofS. aureus
and MRSA from blood cultures.
Staphylococcus aureus septicemia is associated with high
mortality rates, prolonged hospitalization, and increased costs (3, 5). The prevalence of S. aureus septicemia is increasing, primarily due to infections caused by methicillin (meticillin)-resistantS. aureus(MRSA) (20). Several studies have shown that mortality rates among patients suffering from MRSA sep-ticemia is significantly higher than those of patients suffering from infections caused by methicillin-susceptible S. aureus
(MSSA) (5, 18, 19).
The early selection of an appropriate antibiotic regime for the treatment of MSSA or MRSA is crucial for the patient’s outcome (4, 14, 15). However, bacterial identification and preliminary antibiotic susceptibility testing by standard micro-biological procedures still requires 24 to 48 h after growth detection by automated incubation systems. In contrast, new real-time PCR-based methods that use samples directly from positive blood culture bottles allows differentiation of MSSA, MRSA, and coagulase-negative staphylococci (CoNS) within 1.5 to 3 h (7, 12, 13, 16). Such tests promote an early appro-priate antibiotic selection, thus avoiding the unnecessary use of vancomycin, and they reduce mortality, the length of hospital-ization, and costs associated with bloodstream infections caused by these bacteria (3).
We described recently a real-time PCR method for the de-tection of MSSA, MRSA, and CoNS directly from positive blood cultures; it turned out to have 100% sensitivity and 100% specificity for the detection of MSSA and MRSA (7). In this study, the differentiation between MSSA and MRSA directly from signal-positive blood cultures was achieved by the sepa-rate detection of theS. aureus-specific chromosomal fragment
sa442 and the mecA gene (encoding methicillin resistance).
However, since this test is not a commercialized system and does not run on a common platform like, e.g., the SmartCycler (Cepheid, Sunnyvale, CA), its widespread application is lim-ited. Moreover, in blood cultures containing a mixture of MSSA (sa442⫹ but mecA negative) and methicillin-resistant CoNS (MR-CoNS; sa442 negative but mecA⫹), the test is prone to lead to the incorrect identification of MRSA (sa442⫹
mecA⫹).
The BD GeneOhm StaphSR assay (BD Diagnostics GeneOhm, Que´bec, Canada) provides a rapid, simple, commercially avail-able diagnostic test that runs on the SmartCycler for the de-tection ofS. aureusand MRSA from nasal swabs, wounds, and blood cultures. This multiplex real-time PCR amplifies an
S. aureus-specific target sequence and a specific target near the
staphylococcal cassette chromosomemec(SCCmec) insertion site and the orfXjunction in MRSA, thereby differentiating between MSSA and MRSA (9, 17).
Using the herein-described setting, we evaluated the BD GeneOhm StaphSR assay and the PCR that detectssa442and
mecA (designated sa442-mecA–PCR) for the detection of MSSA and MRSA directly from spiked blood cultures.
* Corresponding author. Mailing address: Institut fu¨r Medizinische Mikrobiologie und Krankenhaushygiene, Klinikum der Johann Wolf-gang Goethe-Universita¨t, Paul Ehrlich-Str. 40, D-60596 Frankfurt am Main, Germany. Phone: 49-69-6301-5019. Fax: 49-69-6301-83438. E-mail: [email protected].
䌤Published ahead of print on 15 April 2009.
1689
on May 16, 2020 by guest
http://jcm.asm.org/
MATERIALS AND METHODS
Staphylococcussp. blood culture isolates.In this study, randomly selected and
nonduplicatedStaphylococcusspp. (n⫽109) were included that originally were
isolated from signal-positive blood culture bottles that had been submitted for
routine microbiological diagnostics. MSSA isolates (n⫽45) were isolated
be-tween October 2006 to January 2008, MRSA isolates (n⫽45) from December
2004 to February 2008, and CoNS isolates (n⫽19) from June 2006 to January
2008. All isolates were subjected to our collection of blood culture isolates.
Among the CoNS isolates tested wereStaphylococcus epidermidis (n⫽12),
Staphylococcus capitis(n⫽2),Staphylococcus haemolyticus(n⫽2), Staphylo-coccus hominis(n⫽2), andStaphylococcus warneri(n⫽1).
AllStaphylococcussp. isolates were identified by standard laboratory methods (e.g., DNase testing, mannitol and glucose fermentation, and the latex slide agglutination test; Staphytect Plus; Oxoid, Basingstoke, United Kingdom) and by
the Vitek2 or API Staph system (bioMe´rieux, Nu¨rtingen, Germany).
Addition-ally and as described below, bacterial isolates were analyzed by thesa442-mecA–
PCR (7).
Spiking of blood culture bottles with definedStaphylococcussp. isolates. Staph-ylococcussp. isolates were thawed and cultivated for 24 h on Columbia agar supplemented with 5% sheep blood (BD Diagnostics, Heidelberg, Germany) at
37°C under aerobic conditions. Blood was taken from volunteers (S. Gro¨bner
and V. Kempf), and clotting was avoided by the addition of EDTA. Aerobic blood culture bottles (BACTEC Plus Aerobic/F; BD Diagnostics) were spiked with 5 ml of blood and the respective bacterial isolates. For this purpose, the tip of an 18-gauge needle, attached to a blood-filled 5-ml syringe, was dipped into a corresponding bacterial colony prior to the inoculation of the blood culture bottle. After incubation in a BACTEC-9240 apparatus (BD Diag-nostics), an aliquot from each positive blood culture was taken for (i) Gram staining, (ii) PCR analysis using the BD GeneOhm StaphSR assay (BD
Diag-nostics GeneOhm), (iii) PCR analysis using thesa442-mecA–PCR method (7),
and (iv) subcultivation on Columbia agar plates for routine laboratory identifi-cation (as described above).
sa442-mecAreal-time PCR.sa442-mecAreal-time PCR from positive blood culture bottles was performed as recently described (7). Briefly, 8 ml of positive blood culture was transferred into a BD Vacutainer SST II Advance tube (BD Diagnostics). After centrifugation, DNA was extracted from the supernatant,
and 2l of the extracted DNA was added directly into a LightCycler tube to 18
l of the amplification mixture. Real-time PCRs were performed using a
Light-Cycler (Roche, Mannheim, Germany).
BD GeneOhm StaphSR assay.When a blood culture was flagged positive by the BACTEC-9240, indicating bacterial growth, a Gram stain was performed to confirm the presence of gram-positive cocci in clusters. BD GeneOhm StaphSR
was performed according to the manufacturer’s instructions. Briefly, 2l of the
culture broth was transferred to the sample buffer tube. After being vortexed for
15 s, 50l of the sample suspension was transferred into a lysis tube, vortexed for
5 min, spun quickly to centrifuge down solid contents, and heated at 95°C for 2 min. The lysed samples were kept on ice until further use. The master mix was
reconstituted with 225l diluent and aliquoted (each 25l) into SmartCycler
tubes (Cepheid, Sunnyvale, CA). Next, 3l of each of the lysed samples was
added to the SmartCycler tubes. Positive controls provided by the test kit and negative controls (sample buffer) were included in each run. SmartCycler tubes were centrifuged with a quick spin at 4°C. Finally, the assay was run on the SmartCycler using the manufacturer’s amplification protocol. To work up
po-tentially discrepant results, processed lysis tubes were frozen at⫺80°C.
The PCR results for the BD GeneOhm StaphSR assay were interpreted using the SmartCycler software (SmartCyclerDX software, version 1.7b), which
deliv-ered the following test results: negative (neitherS. aureusnor MRSA DNA was
detected), reactive (S. aureusDNA was detected), or positive (MRSA DNA was
detected).
Additional analysis of isolates with discrepant results in the BD GeneOhm StaphSR assay.For the samples for which the BD GeneOhm StaphSR assay
results did not agree with those of thesa442-mecA–PCR, the BD GeneOhm
StaphSR assay was repeated with aliquots from the initial blood culture and, additionally, with the respective bacterial isolates grown on Columbia agar by inoculating a respective colony into the BD GeneOhm StaphSR sample buffer. Moreover, bacterial subcultivation on CHROMagar MRSA plates (Becton Dick-inson), antibiotic testing (Vitek2) for methicillin resistance using a microdilution method according to the recommendations of the Clinical and Laboratory
Stan-dards Institute (CLSI) (2), andspatyping (8) were performed. In addition, these
isolates were tested for the presence of the penicillin binding protein 2⬘by using
an immunoassay (PBP2⬘test kit; Oxoid, Basingstoke, United Kingdom).
mecAgene PCR analysis.The presence or absence of themecAgene was
determined by the analysis ofStaphylococcussp. DNA by an additional PCR
assay specific to themecAgene (11). Here, 1l of bacterial DNA was added to
19l of the PCR mixture. PCR amplification products were analyzed on 2%
agarose gels. The size of themecA-PCR product was 174 bp; positive (MRSA)
and negative (MSSA) controls were included in each run (data not shown). SCCmectyping.The following methods were used for the SSCmectyping of
the discrepantS. aureusisolates. For the identification of the SCCmectype, the
lysates first were analyzed with two multiplex PCR assays to determine themec
complex class, A, B, or C (1), and with a multiplex PCR to determine theccr
complex based on a method described before (10). In both assays, 1l of each
DNA sample was added to 49l of PCR mixture, and PCRs were performed
using a PTC-200 thermal cycler (Bio-Rad, Hercules, CA). PCR amplification products were analyzed on 1% agarose gels (data not shown). Additionally, the
presence of SCCmectypes I to V was determined by a multiplex PCR based on
a method described previously (21). Here, 2l of each DNA sample was added
to 23l of PCR mixture. PCR amplification products were analyzed on a 1%
agarose gel (data not shown).
RESULTS
Analysis of blood cultures spiked with one Staphylococcus
[image:2.585.44.546.91.170.2]species per bottle. To evaluate the BD GeneOhm StaphSR assay in comparison to thesa442-mecA–real-time PCR assay, 109 signal-positive blood cultures, each spiked with one par-ticularStaphylococcussp. blood culture isolate, were analyzed in parallel in both assays. At the time of sample preparation, all signal-positive blood cultures showed the growth of gram-pos-itive cocci in clusters when analyzed by Gram staining and, accordingly, all bacterial isolates exhibited the typical pheno-typic characteristics when undergoing standard laboratory identification (e.g., DNase, the expression of clumping factor, etc.; data not shown). All S. aureus isolates (45 MSSA, 45 MRSA) were correctly identified by the sa442-mecA–PCR method (Table 1). However, the BD GeneOhm StaphSR assay repeatedly identified three of the MSSA isolates as MRSA and two MRSA isolates as S. aureus (but not as MRSA) when
TABLE 1. Evaluation of the BD GeneOhm StaphSR assay andsa442-mecAreal-time PCR for the detection of MSSA, MRSA, and CoNS in blood cultures spiked with defined blood culture isolates
Isolate type (n)
No. detected by BD GeneOhm StaphSR No. detected bymecA-sa442–PCR
Negative (CoNS)
Reactive (S. aureus)
Positive (MRSA)
sa442negative,mecA
negative (CoNS)
sa442negative,
mecA⫹(CoNS)
sa442⫹,mecA
negative (MSSA)
sa442⫹,mecA⫹
(MRSA)
MSSA (45) 0 42 3a 0 0 45 0
MRSA (45) 0 2b 43 0 0 0 45
CoNS (19) 19 0 0 11 8 0 0
Total (109) 19 44 46 11 8 45 45
aThree MSSA isolates were incorrectly identified as MRSA by the BD GeneOhm StaphSR assay.
bTwo MRSA isolates were not identified as MRSA by the BD GeneOhm StaphSR assay.
on May 16, 2020 by guest
http://jcm.asm.org/
tested directly from blood cultures. None of the 19 CoNS was misidentified in either assay, excluding the presence ofS. au-reusin these samples (Table 1). In summary, the sensitivity and specificity of the BD GeneOhm StaphSR assay was 100% each (95% confidence interval [CI], 96.0 to 100% and 82.4 to 100%, respectively) for the detection ofS. aureus(n⫽90), including MSSA (n ⫽ 45) and MRSA (n ⫽45). For the detection of MRSA (n⫽45), the test was 95.6% (43/45) sensitive (95% CI, 84.9 to 99.5%) and 95.3% (61/64) specific (95% CI, 86.9 to 99.0%).
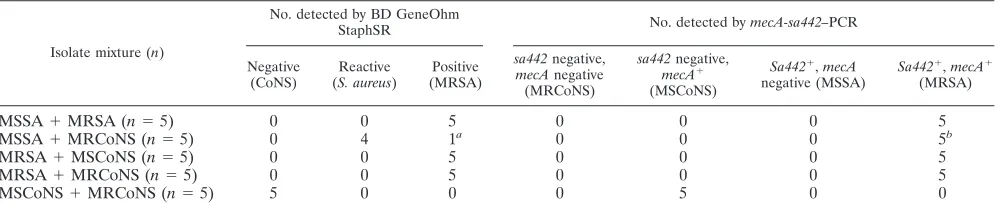
Analysis of blood culture bottles spiked with mixtures of staphylococcal isolates.To evaluate the BD GeneOhm StaphSR assay for its use in positive blood cultures in greater detail, blood culture bottles were spiked with two different staphylo-coccal isolates (Table 2). This setting mimics a polymicrobial septicemia prone to deliver incorrect results in rapid molecular diagnostics.
All mixtures of MSSA and MRSA (n⫽ 5) were identified correctly as MRSA-containing samples by both assays. Since the BD GeneOhm StaphSR assay targets a specific sequence for MRSA and a specific sequence forS. aureusin the same reaction, the assay will report MRSA in the case of mixed MSSA and MRSA cultures; therefore, the appraisal of the result MRSA gets priority over the appraisal of S. aureus. Similarly, thesa442-mecA–PCR assay (detectingsa442 as an
S. aureus-specific sequence and mecA coding for methicillin
resistance) leads to the identification as MRSA and neglects the presence of MSSA in the same sample.
Thesa442-mecA–PCR assay suffers from potentially
incor-rect MRSA detection, as this assay detects theS. aureus -spe-cificsa442gene and themecAgene encoding methicillin resis-tance in two single PCRs. Therefore, in blood cultures containing both MSSA andmecA-positive methicillin-resistant CoNS (MRCoNS), this approach might lead to the incorrect diagnosis of MRSA, and this is a known limitation of the method. Indeed, due to the simultaneous detection of the
sa442and mecAgenes from two independent staphylococcal
genomes, thesa442-mecA–PCR setting leads to the incorrect diagnosis of MRSA (sa442⫹mecA⫹) in such mixtures (n⫽5) (Table 2).
In contrast, the BD GeneOhm StaphSR assay correctly iden-tified four of the MSSA isolates from mixtures of MSSA and MRCoNS. One mixture of MSSA and MRCoNS was identified as MRSA by the BD GeneOhm StaphSR assay. However, this
particular MSSA-MRCoNS mixture contained one of those three MSSA isolates that were misidentified as MRSA (isolate 114; see below). Therefore, the diagnosis of MRSA resulted from the MSSA falsely detected as MRSA and not from the MRCoNS.
Mixtures containing (i) MRSA and methicillin-susceptible CoNS (MSCoNS) (n⫽5), (ii) MRSA and MRCoNS (n⫽5), and (iii) MSCoNS and MRCoNS (n ⫽5) all were correctly identified in both assays (Table 2).
Analysis ofS. aureus isolates with discrepant results with the BD GeneOhm StaphSR assay.Isolates 13, 30, and 114 (all MSSA; evaluated by conventional laboratory methods and by using thesa442-mecA–PCR from a singular bacterial colony) were repeatedly identified as MRSA by the BD GeneOhm StaphSR assay when performed directly from positive blood cultures. Furthermore, isolates 35 and 126 (both MRSA) were identified asS. aureusand not MRSA by the BD GeneOhm StaphSR assay when repeatedly tested directly from blood culture (Table 3). In contrast, when tested from singular bac-terial colonies grown on Columbia agar plates (not recom-mended by the manufacturer for routine diagnostics; per-formed only for internal purposes during our investigations), isolate 126 was correctly identified as MRSA, whereas isolate 35 still was identified asS. aureusand not as MRSA.
Misidentified MSSA isolates.Isolates 13, 30, and 114 were correctly identified as MSSA by thesa442-mecA–PCR setting
(sa442⫹andmecAnegative) but were identified to be MRSA
with the BD GeneOhm StaphSR assay. Moreover, all three isolates were susceptible for oxacillin tested by microdilution test, no growth was observed on oxacillin-containing Mueller-Hinton agar plates and CHROMagar MRSA plates, and the PBP2⬘ test was negative (Table 3; not all data are shown). Accordingly, mecA-specific PCRs (11) were negative for all three isolates, confirming the absence of a functional mecA
gene (data not shown). Those isolates turned out to represent revertant strains in which a part of the SCC (including the
mecAgene) was deleted. All three strains were not typeable by SCCmec multiplex PCRs (data not shown) and belonged to different spa types (Table 3), indicating that there was no epidemiological relationship among those isolates.
Misidentified MRSA isolates. Strains 35 and 126 (both MRSA; identified by the sa442-mecA–PCR setting [sa442⫹ mecA⫹] and by the described conventional identification
tech-TABLE 2. Evaluation of the BD GeneOhm StaphSR andsa442-mecAreal-time PCR for the detection of MSSA, MRSA, MSCoNS, or MRCoNS in blood cultures spiked with defined mixtures of blood culture isolates
Isolate mixture (n)
No. detected by BD GeneOhm
StaphSR No. detected bymecA-sa442–PCR
Negative (CoNS)
Reactive (S. aureus)
Positive (MRSA)
sa442negative,
mecAnegative
(MRCoNS)
sa442negative,
mecA⫹
(MSCoNS)
Sa442⫹,mecA
negative (MSSA)
Sa442⫹,mecA⫹
(MRSA)
MSSA⫹MRSA (n⫽5) 0 0 5 0 0 0 5
MSSA⫹MRCoNS (n⫽5) 0 4 1a 0 0 0 5b
MRSA⫹MSCoNS (n⫽5) 0 0 5 0 0 0 5
MRSA⫹MRCoNS (n⫽5) 0 0 5 0 0 0 5
MSCoNS⫹MRCoNS (n⫽5) 5 0 0 0 5 0 0
a
In this mixture, one MSSA isolate was incorrectly identified as MRSA by the BD GeneOhm StaphSR assay.
b
In these mixtures, incorrect results (MRSA) were generated using thesa442-mecA–PCR.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.44.542.90.194.2]niques; Table 3) were identified asS. aureusand not as MRSA with the BD GeneOhm StaphSR assay.
By SCCmectyping, isolates 35 and 126 were identified as MRSA SCCmectype II (data not shown). A specific multiplex PCR designed to detect MRSA strains of low prevalence (which are not covered by the BD GeneOhm StaphSR assay) revealed that isolates 35 and 126 were MRSA (data not shown). Discordantly with the results from blood culture bot-tles, isolate 126 was identified correctly as MRSA with the BD GeneOhm StaphSR assay when tested with colonies grown on agar plates (Table 3).
DISCUSSION
This report describes, for the first time, the evaluation of the BD GeneOhm StaphSR assay for detecting MSSA (based on the detection ofS. aureusnot being MRSA) and MRSA from spiked positive blood cultures in direct com-parison with another rapid molecular approach, the sa442-mecA–PCR assay, which recently was analyzed by us for its potential use in the rapid molecular identification of staph-ylococci from blood cultures (7). Since the number of MRSA blood culture isolates at our hospital is relatively low (⬃20 per year), we performed the herein-described study with spiked blood cultures from our collection of blood culture isolates. In total, we analyzed 134 blood cultures, of which 45 were spiked with MSSA isolates, 45 with MRSA isolates, 19 with CoNS, and 25 with mixtures of staphylo-cocci. When blood cultures were spiked with CoNS, none of these assays led to incorrect results. Using thesa442-mecA– PCR assay, all blood cultures spiked with singular MSSA or MRSA isolates were correctly identified. In contrast, five discrepant results arose by using the BD GeneOhm StaphSR assay. When analyzing mixtures of staphylococci, both assays revealed a good reliability influenced by the specific limitations of each assay.
Three MSSA strains (13, 30, and 114) were misidentified as MRSA by the BD GeneOhm StaphSR assay. None of these strains harbored a functionalmecAgene as analyzed by PCR techniques, and no SCCmectype could be determined. Inter-estingly, the analysis of these results (MSSA strains that appear to be mecA negative but BD GeneOhm StaphSR positive) revealed that these three isolates represent MRSA revertant strains, and this explains on a molecular basis why these MSSA isolates were reactive in the BD GeneOhm StaphSR assay, leading to the misidentification as MRSA (data not shown). Knowing that themecAgene is carried by the SCCmecand that the MRSA target of the BD GeneOhm StaphSR assay is lo-cated in the 3⬘sequence downstream of SCCmec, these results suggest that the revertant isolates (13, 30, and 114) harbor residual fragments of themecright-extremity junction belong-ing to the SCCmeccassette. SCCs are mobile elements that are able to insert into and be excised from the chromosome. Such excision of the SCCmeccan be complete or partial; in the latter case, some fragments can be left at the integration site of the SCCmec(6). Therefore, residual SCCmecextremity fragments containing such MRSA target sequences most likely are the molecular reason for the misidentification of these three MSSA isolates.
Two MRSA strains (35 and 126) were identified asS. aureus
TABLE 3. Analysis of the isolates with discrepant results in BD GeneOhm StaphSR, Sa442 -mecA –PCR, and phenotypic testing Isolate no. (type) Real-time PCR result directly from blood culture Isolate analysis (subcultivation of positive blood culture on agar plates) Final assignment BD GeneOhm StaphSR sa442-mecA BD GeneOhm StaphSR sa442-mecA OX a MIC ( g/ml) by Vitek2 Growth in CHROMagar PBP2 ⬘ latex test result spa type SCC mec type 13 (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) ⱕ 0.25 No ⫺ t002 Nontypeable Revertant MRSA strain b 30 (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) ⱕ 0.25 No ⫺ t127 Nontypeable Revertant MRSA strain b 114 (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) Positive (MRSA) ⫹ / ⫺ (MSSA) ⱕ 0.25 No ⫺ t004 Nontypeable Revertant MRSA strain b 35 (MRSA) Reactive ( S. aureus ) ⫹ / ⫹ (MRSA) Reactive ( S. aureus ) ⫹ / ⫹ (MRSA) ⱖ 4 Yes ⫹ t002 II MRSA (undetected by BD GeneOhm StaphSR assay) 126 (MRSA) Reactive ( S. aureus ) ⫹ / ⫹ (MRSA) Positive (MRSA) ⫹ / ⫹ (MRSA) ⱖ 4 Yes ⫹ t002 II MRSA (undetected by BD GeneOhm StaphSR assay) aOX, oxacillin. bCharacterized by the absence of mecA and the detection of residual fragments of the SCC mec containing BD GeneOhm StaphSR target sequences.
on May 16, 2020 by guest
http://jcm.asm.org/
but not as MRSA by the BD GeneOhm StaphSR assay from blood cultures. When tested from colonies grown on agar plates (not recommended by the manufacturer; performed only for internal purposes during this investigation), strain 35 still was identified asS. aureus(and not as MRSA), whereas for strain 126 the result changed to MRSA. The molecular expla-nation for this phenomenon remains unclear. Most probably, the identification as MRSA from culture has to be judged as an incidental correct identification of this particular isolate based on an unspecific amplification of the MRSA-specific sequences (intellectual property of BD GeneOhm, details not shown). Misidentifications occurring with the BD GeneOhm StaphSR assay can be explained by the fact that the assay was designed to detect the most common MRSA strains. However, a minor population of MRSA strains cannot be identified, because the specific DNA sequence is not targeted by the BD GeneOhm StaphSR assay; in fact, isolates 35 and 126 were such rare strains. Considering that these strains represent only a minor population of all MRSA strains (data not shown), the detec-tion of MRSA in blood cultures by the BD GeneOhm StaphSR technology represents a reasonable trade off between prac-ticability and correct MRSA identification. However, these results also imply that the rapid detection of MRSA or MSSA by the BD GeneOhm StaphSR assay nevertheless should be followed up by conventional culture-based labo-ratory methods, which still are necessary for antimicrobial susceptibility testing.
When the two methods are compared to each other, the advantage of thesa442-mecAreal-time PCR method is obvi-ously its higher specificity for the detection of MRSA. Al-though this assay is predisposed to deliver incorrect results in the detection of MRSA in mixtures of MSSA and MRCoNS, we did not observe such incorrect identification results until now in our routine laboratory. The reason for this fact most likely is that mixed staphylococcal blood cultures are rare in our hospital: such mixtures did not appear in a former study with 475 routine blood cultures (7). Nevertheless, this limita-tion of the sa442-mecA–PCR assay is overcome by the BD GeneOhm StaphSR assay. The latter delivers the correct iden-tification of MSSA and MRSA even in mixed-blood cultures containingS. aureusand MRCoNS, since the precondition for the diagnosis of MRSA by this assay is the simultaneous am-plification of a target near the SCCmecinsertion site and the
S. aureus-specific orfXjunction. Moreover, this assay is very
rapid (⬃1.5 h) and easy to perform in laboratories where the SmartCycler apparatus has already been implemented for other applications.
In summary, both herein-described real-time PCR methods (BD GeneOhm StaphSR assay andsa442-mecA–PCR assay) are reliable, useful tools for the detection of MSSA and MRSA directly from positive blood cultures. Even though studies have shown that revertant strains and MRSA strains undetected by the BD GeneOhm StaphSR assay are rare (data collected during the BDGeneOhm StaphSR clinical study showed that the prevalence of revertant strains represents less than 1% of the specimens tested), their occurrence currently is being mon-itored and will be taken into consideration when improving the BD GeneOhm StaphSR assay in the future.
ACKNOWLEDGMENTS
We thank Mariola Gwodz, Kerstin Kro¨mer, Cornelia Lu¨th, and Stefanie Richt (Tu¨bingen, Germany) for excellent technical assis-tance.
REFERENCES
1.Chongtrakool, P., T. Ito, X. X. Ma, Y. Kondo, S. Trakulsomboon, C. Tien-sasitorn, M. Jamklang, T. Chavalit, J. H. Song, and K. Hiramatsu.2006.
Staphylococcal cassette chromosomemec(SCCmec) typing of
methicillin-resistant Staphylococcus aureusstrains isolated in 11 Asian countries: a
proposal for a new nomenclature for SCCmecelements. Antimicrob. Agents
Chemother.50:1001–1012.
2.CLSI.2008. Performance standards for antimicrobial susceptibility testing; 18th informational supplement, vol. 27. Clinical and Laboratory Standards Institute, Wayne, PA.
3.Cosgrove, S. E.2006. The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs.
Clin. Infect. Dis.42(Suppl. 2):S82–S89.
4.Cosgrove, S. E., and V. G. Fowler, Jr.2008. Management of
methicillin-resistantStaphylococcus aureusbacteremia. Clin. Infect. Dis.46(Suppl. 5):
S386–S393.
5.Cosgrove, S. E., G. Sakoulas, E. N. Perencevich, M. J. Schwaber, A. W. Karchmer, and Y. Carmeli.2003. Comparison of mortality associated with
methicillin-resistant and methicillin-susceptibleStaphylococcus aureus
bac-teremia: a meta-analysis. Clin. Infect. Dis.36:53–59.
6.Donnio, P. Y., F. Fevrier, P. Bifani, M. Dehem, C. Kervegant, N. Wilhelm, A. L. Gautier-Lerestif, N. Lafforgue, M. Cormier, and C. A. Le.2007. Mo-lecular and epidemiological evidence for spread of multiresistant
methicillin-susceptibleStaphylococcus aureusstrains in hospitals. Antimicrob. Agents
Chemother.51:4342–4350.
7.Gro¨bner, S., and V. A. Kempf.2007. Rapid detection of methicillin-resistant staphylococci by real-time PCR directly from positive blood culture bottles.
Eur. J. Clin. Microbiol. Infect. Dis.26:751–754.
8.Harmsen, D., H. Claus, W. Witte, J. Rothga¨nger, H. Claus, D. Turnwald, and U. Vogel.2003. Typing of methicillin-resistantStaphylococcus aureusin a
university hospital setting by using novel software forsparepeat
determina-tion and database management. J. Clin. Microbiol.41:5442–5448.
9.Huletsky, A., R. Giroux, V. Rossbach, M. Gagnon, M. Vaillancourt, M. Bernier, F. Gagnon, K. Truchon, M. Bastien, F. J. Picard, A. van Belkum, M. Ouellette, P. H. Roy, and M. G. Bergeron.2004. New real-time PCR assay for
rapid detection of methicillin-resistantStaphylococcus aureusdirectly from
specimens containing a mixture of staphylococci. J. Clin. Microbiol.42:1875–
1884.
10.Kondo, Y., T. Ito, X. X. Ma, S. Watanabe, B. N. Kreiswirth, J. Etienne, and K. Hiramatsu.2007. Combination of multiplex PCRs for staphylococcal
cassette chromosomemectype assignment: rapid identification system for
mec,ccr, and major differences in junkyard regions. Antimicrob. Agents
Chemother.51:264–274.
11.Martineau, F., F. J. Picard, N. Lansac, C. Menard, P. H. Roy, M. Ouellette, and M. G. Bergeron.2000. Correlation between the resistance genotype determined by multiplex PCR assays and the antibiotic susceptibility patterns ofStaphylococcus aureusandStaphylococcus epidermidis. Antimicrob. Agents
Chemother.44:231–238.
12.Paule, S. M., A. C. Pasquariello, R. B. Thomson, Jr., K. L. Kaul, and L. R. Peterson.2005. Real-time PCR can rapidly detect methicillin-susceptible
and methicillin-resistantStaphylococcus aureusdirectly from positive blood
culture bottles. Am. J. Clin. Pathol.124:404–407.
13.Ruimy, R., M. Dos-Santos, L. Raskine, F. Bert, R. Masson, S. Elbaz, C. Bonnal, J. C. Lucet, A. Lefort, B. Fantin, M. Wolff, M. Hornstein, and A. Andremont.2008. Accuracy and potential usefulness of triplex real-time PCR for improving antibiotic treatment of patients with blood cultures showing clustered gram-positive cocci on direct smears. J. Clin. Microbiol.
46:2045–2051.
14.Small, P. M., and H. F. Chambers.1990. Vancomycin forStaphylococcus aureusendocarditis in intravenous drug users. Antimicrob. Agents
Che-mother.34:1227–1231.
15.Stryjewski, M. E., L. A. Szczech, D. K. Benjamin, Jr., J. K. Inrig, Z. A. Kanafani, J. J. Engemann, V. H. Chu, M. J. Joyce, L. B. Reller, G. R. Corey, and V. G. Fowler, Jr.2007. Use of vancomycin or first-generation cephalo-sporins for the treatment of hemodialysis-dependent patients with
methicil-lin-susceptibleStaphylococcus aureusbacteremia. Clin. Infect. Dis.44:190–
196.
16.Thomas, L. C., H. F. Gidding, A. N. Ginn, T. Olma, and J. Iredell.2007.
Development of a real-timeStaphylococcus aureusand MRSA (SAM-) PCR
for routine blood culture. J. Microbiol. Methods68:296–302.
17.Warren, D. K., R. S. Liao, L. R. Merz, M. Eveland, and W. M. Dunne, Jr.
2004. Detection of methicillin-resistantStaphylococcus aureusdirectly from
nasal swab specimens by a real-time PCR assay. J. Clin. Microbiol.42:5578–
5581.
18.Weinstein, M. P., M. L. Towns, S. M. Quartey, S. Mirrett, L. G. Reimer, G. Parmigiani, and L. B. Reller.1997. The clinical significance of positive blood
on May 16, 2020 by guest
http://jcm.asm.org/
cultures in the 1990s: a prospective comprehensive evaluation of the micro-biology, epidemiology, and outcome of bacteremia and fungemia in adults.
Clin. Infect. Dis.24:584–602.
19.Wisplinghoff, H., T. Bischoff, S. M. Tallent, H. Seifert, R. P. Wenzel, and M. B. Edmond.2004. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study.
Clin. Infect. Dis.39:309–317.
20.Wyllie, D. H., D. W. Crook, and T. E. Peto.2006. Mortality after Staphylo-coccus aureusbacteraemia in two hospitals in Oxfordshire, 1997–2003:
co-hort study. BMJ333:281.
21.Zhang, K., J. A. McClure, S. Elsayed, T. Louie, and J. M. Conly.2005. Novel multiplex PCR assay for characterization and concomitant subtyping of
staphylococcal cassette chromosomemectypes I to V in methicillin-resistant
Staphylococcus aureus. J. Clin. Microbiol.43:5026–5033.